Chronic obstructive pulmonary disease (COPD) is an important and a growing cause of morbidity and mortality worldwide. Cardiovascular, musculoskeletal, metabolic, and mental comorbidities are considered to be part of the frequently prevalent non-pulmonary sequelae of the disease.1,2 Increasing evidence suggests that extra-pulmonary effects of COPD and airflow limitation are only poorly correlated.3 Waschki, et al. found that objectively measured physical activity is the strongest predictor of all-cause mortality in patients with COPD.4
The association between physical inactivity and poor outcomes are well established for patients with pulmonary disease, cardiac disease, chronic kidney disease.4,5,6 Patients with pulmonary disease, cardiac disease, or renal disease typically engage in a lower level of physical activity than do the general population, which can induce a catabolic state including reduced neuromuscular functioning, reduced exercise tolerance and reduced cardiorespiratory fitness (CRF).
CRF is an important consideration, in addition to physical activity, as it is a strong predictor of mortality; low CRF presents a particularly high risk of death compared to other common risk factors, such as diabetes, high cholesterol or hypertension.7 CR fitness is defined as the ability of the circulatory and respiratory systems to supply oxygen during sustained physical activity and is usually expressed as maximal oxygen uptake ( O2max) during maximal exercise testing.8 In 2016, the American Heart Association published a scientific statement9 recommending that CRF, quantifiable as O2max, be regularly assessed and utilized as a clinical vital sign. This statement was based on mounting evidence that lower CRF levels are associated with high risk of cardiovascular disease, all-cause mortality, and mortality rates stemming from various types of cancers.
O2max) during maximal exercise testing.8 In 2016, the American Heart Association published a scientific statement9 recommending that CRF, quantifiable as O2max, be regularly assessed and utilized as a clinical vital sign. This statement was based on mounting evidence that lower CRF levels are associated with high risk of cardiovascular disease, all-cause mortality, and mortality rates stemming from various types of cancers.
O2max is expressed either as an absolute rate in (for example) liters of oxygen per minute (L/min) or as a relative rate in (for example) milliliters of oxygen per kilogram of body mass per minute (e.g., mL/(kg•min)). The latter expression is often used to compare the performance of endurance athletes and patients.
Figure shows gas transport mechanisms for coupling cellular (internal) to pulmonary (external) respiration. The gears represent the functional interdependence of the physiological components of the system. Cardiac output, pulmonary diffusion capacity, oxygen carrying capacity, renal function and other peripheral limitations like muscle diffusion capacity, mitochondrial enzymes, and capillary density are all examples of O2max determinants.
Figure. Gas Transport Mechanisms for Coupling Cellular to Pulmonary Respiration: Five Major Determinants for O2max
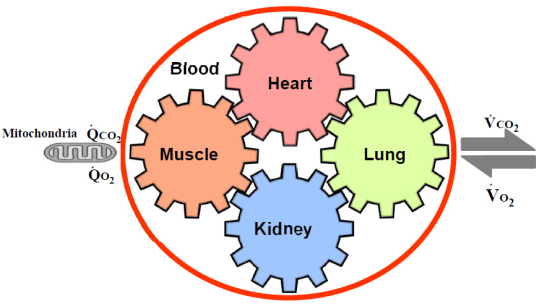
The large increase in O2 utilization by the muscles (QO2) is achieved by increased extraction of O2 from the blood perfusing the muscles, the dilatation of selected peripheral vascular beds, an increase in cardiac output (stroke volume and heart rate), an increase in pulmonary blood flow by recruitment and vasodilatation of pulmonary blood vessels, and finally, an increase in ventilation. O2 is taken up (O2) from the alveoli in proportion to the pulmonary blood flow and degree of O2 desaturation of hemoglobin in the pulmonary capillary blood. Metabolic acidosis in chronic kidney disease (CKD) patients promote muscle protein wasting and protein-energy wasting (PEW) by increasing protein degradation10 and reducing protein synthesis.11 As a result, maintenance of muscle mass is impaired in CKD patients with altered protein turnover rates.12 Adding to sarcopenia, metabolic acidosis, protein-energy wasting, angiotensin II, myostatin overexpression in uremia contribute the etiology for muscle wasting in CKD.13 Moreover, the drug erythropoietin (EPO) can boost O2max by a significant amount in both humans and other mammals.14
COPD often coexists with other diseases (comorbidities such as heart disease, CKD, osteoporosis) that may have a significant impact on prognosis. Thirty-three percent of elderly patients with heart failure had COPD and 25% of elderly patients with COPD also had heart failure.15 This risk of comorbid disease can be increased by the sequelae of COPD; e.g., reduced physical activity. As super-aged society has come, the number of persons with multimorbidity and multiple disabilities (MMD)16 and their needs of rehabilitation have increased rapidly more than we have expected.16 O2max offers the investigator the unique opportunity to study simultaneously the cellular, cardiovascular, ventilatory and metabolic systems’ responses under conditions of precisely controlled stress. This is of significant practical importance because O2max measured by cardiopulmonary exercise testing, provides what is probably the most sensitive assessment of the effect of new therapy on function of any diseased organ system whose major function is to couple pulmonary gas exchange to cellular respiration. For example, it is important to determine whether new medical, surgical, and rehabilitative procedures can effectively intervene to improve the gas transport capability of a diseased organ system.



