CASE REPORT
We report a case of gastric diverticulum misdiagnosed as a left adrenal lesion on both ultrasound and CT imaging and later identified on a follow-up CT.
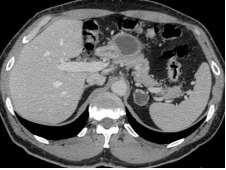
A 56 year-old man with a history of gastroesophageal reflux disease was admitted to our Hospital with left abdominal pain. There was no history of vomiting, hematemesis, melena, tiredness or jaundice. Bowel sounds were normal and no masses were identified at clinical examination. An ultrasound abdominal scan was performed and a hypoechoic 24 mm mass in left adrenal loggia was reported. An abdominal CT scan showed a 2.4 cm rounded mass in the area of the left adrenal gland with densitometric mean values of -7 HU, interpreted as adrenal adenoma (Figure 1). In the following days the patient underwent a complete endocrinological evaluation that showed normal findings with normal adrenal function; ACTH level and urinary catecholamines were both within normal range. The patient was then discharged and scheduled for a follow-up CT.
Figure 1: Axial contrast- enhanced CT image showing a rounded lesion interpreted as the upper portion of the left adrenal gland with sharp edges and weak parietal enhancement.
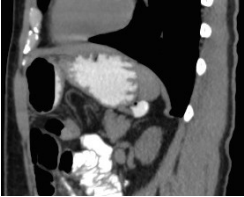
After 6 months the patient underwent a second follow-up CT that showed a little intralesional gas bubble (Figure 2); CT scan was subsequently repeated after oral administration of contrast medium (Gastrografin®); the previously described lesion showed continuity with the gastric wall, contrast medium staining of the lumen lesion with contextual air bubbles suggestive of gastric diverticulum (Figure 3 and 4). Diagnosis was later confirmed by esophagogastroduodenoscopy.
Figure 2: Axial contrast- enhanced CT image showing a gas bubble in the ventral aspect of the suprarenal lesion.

Figure 3: Axial non-enhanced ct image showing an intense lumen staining of both the lesion and the gastric lumen after oral administration of contrast medium.
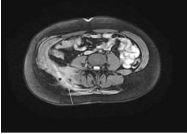
Figure 4: Sagittal reconstruction of the same follow-up ct scan (shown in figure 3) after oral administration of contrast medium.
DISCUSSION
Gastric Diverticulum (GD) is an outpouching of the gastric wall. GDs are rare and they are commonly incidentally detected during diagnostic examinations of the abdomen. Prevalence ranges from 0.04% in upper gastrointestinal tract X-ray examination to 0.01%-0.11% at esophagogastroduodenoscopy.1
GDs are the least common diverticula of the gastrointestinal tract. Two main categories are identified, congenital and acquired. Diverticula of the gastric antrum, prepyloric or pyloric regions are extremely rare and usually asymptomatic. Clinical history may vary from complete absence of symptoms to dyspepsia, to major upper Gastrointestinal (GI) bleeding, making this condition a diagnostic challenge.2
Masses mimicking adrenal tumors appear more frequently on the left side due to the close proximity of the left adrenal gland to different structures such as the gastric fundus, the first loops of the jejunum, the spleen, the pancreas and the left kidney.3 Conditions such as gastric stasis, gastric diverticulum, duplicated bowel loop, accessory spleen, splenic vessels, aneurysm of the splenic artery, portosystemic venous collaterals (in portal hypertension), left renal and pancreatic tumors and submucosal gastric tumor may be difficult to differentiate from left adrenal tumor.4,5
In order to prevent false diagnosis of adrenal tumor on CT, the adrenal region should be scanned with thin slices performed with multirow detector CT with the support of multi-planar reconstruction images. In the case of suspected gastric diverticula, oral administration of contrast medium may be indicated.
In conclusion, on the basis of our experience, the possibility of gastric diverticulum should be taken into consideration in the full differential diagnosis of adrenal masses.
CONFLICTS OF INTERESTS
We declare there are neither conflicts of interest nor acknowledgements’.
CONSENT
No consent is required to our article publication.


