INTRODUCTION
Kidney cysts (KC) include both benign and malignant etiology and can occur spontaneously or be caused by acquired cystic kidney disease, such as polycystic kidney disease (PKD). KC are masses that are predominantly composed of spaces filled with clear or straw-colored fluid.1 Spontaneous perinephric hemorrhage due to KC rupture is uncommon complication but when it occurs can cause an emergency situation that may endanger the patient’s life.
In 1856 Carl Wunderlich first described the condition of spontaneous, non-traumatic renal bleeding confined to the subcapsular and perirenal spaces2 that may present with a classic triad of symptoms knows as “Lenk’s triad”: acute flank or abdominal pain, flank mass and hypovolemic shock. Herein, we report a case of Wunderlich syndrome (WS) due to spontaneous rupture of a simple KC.
CASE REPORT
A 75-year-old man presented to the emergency department with left flank pain that lasted for 5-6 hours. His medical history included hypertension, mitral regurgitation, aspirin therapy, implantation of cardiac pacemaker for an atrioventricular block, infrarenal aorticaneurysm repair, chronic renal failure (serum creatinine 6 mg/L, creatinine clearance sec., CockcroftGault 10 ml/min). He had no history of previous abdominal trauma. Physical examination indicated moderate tenderness across the whole abdomen, which was more evident on the left side. He had a severe hypotension, pulse rate of 92 beats/min, respiratory rate of 24 breaths/min and body temperature of 36.8 °C.
A complete blood count revealed a hemoglobin (Hgb) of 6 g/dL and a severe thrombocytopenia.
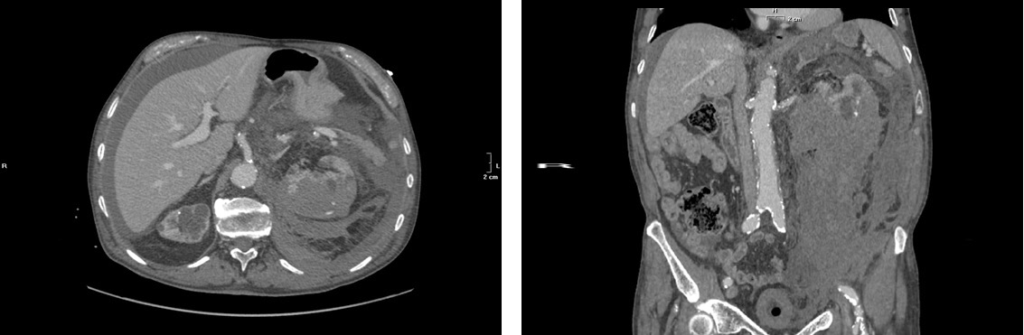
A computed tomography (CT) scan was performed. It showed a retroperitoneal hematoma on left side and left hemoperitoneum extended to the pelvic cavity (Figure 1A and 1B).
Figures 1A and 1B: Hemoperitoneum and a retroperitoneal hematoma on the left side displacing the spleen, the pancreatic tail and intestinal structures, extended to the pelvic cavity
The patient underwent an angiogiography scan showing a hemorrhagic spreading from the left kidney. Due to the rapid worsening of clinical conditions the patient underwent an explorative laparotomy. A large retroperitoneal hematoma extending from the renal region to the pelvis was found and a left nephrectomy was done.
During this surgical manoeuvre an accidental injury of the tail of the pancreas occurred with a modest parenchymal laceration that was immediately sutured. Five hours later, a second explorative laparotomy due to persistent abdominal bleeding and hemodynamic instability was done.
Twenty-four hours later a CT scan angiography showed a modest hemorrhagic spreading from a minor branch of the superior mesenteric artery that was unsuccessfully embolized. Nevertheless, the patient showed a hemodynamic stability which was maintained as such in the following days. A haemodialysis therapy started in the subsequent days.
Histopathological examination described an atrophic kidney end-stage-type with cortico—medullary atrophy, multiple giant cystic lesions without specific coating.
DISCUSSION
The WS is a potentially life threatening condition. In a metaanalysis on spontaneous perirenal hemorrhage, the most common etiology are benign or malignant neoplasms (61%) with angiomyolipoma being predominant (29.1%) followed closely by renal cell carcinoma (26.1%) and vascular disease (17%) with polyarteritis nodosa occurring most frequently (12%).3 This emergency condition may occur with acute flank pain, flank mass and hypovolemic shock in 83%, 19% and 11% respectively.3
In our case, the spontaneous retroperitoneal hemorrage was associated to a probable giant haemorragic cyst that is uncommon since cyst rupture occurs into caliceal system rather than the perinephric space. In this context large KC, hemorrhage and infection and a coexisting urinary tract obstruction are predisposing factors for spontaneous cyst rupture.4
In literature sparse cases of WS due to the non-traumatic rupture of a simple KC were reported. In particular Puerta et al5 described a case of perirenal hematoma due to rupture of a KC in a 50 years old female occurred with pain, a mass in left renal fossa and hypovolemia, who needed surgical drainage of the hematoma without nephrectomy. Finally, Lin et al6 described another case of spontaneous perinephric hemorrhage due a hemorrhagic renal cyst in 46-years-old women that was conservatively treated.
In our case, the presence of hemoperitoneum not allowed a conservative treatment and an explorative laparotomy was mandatory.
CONCLUSION
Wunderlich syndrome after spontaneous, non-traumatic kidney cyst rupture is a rare entity. A multimodality approach is necessary to a have a definitive diagnosis in order to choose the best treatment possible for the patient.
FUNDING
The authors received no financial support for the research, authorship, and/or publication of this article.
CONFLICTS OF INTEREST
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
CONSENT
The patient has provided written permission for the publication of this case details.



