INTRODUCTION
Diabetes mellitus, hypertension, and so on are linked to the obesity and metabolic syndrome. Existing guidelines, however, to help people achieve lifestyle change are difficult to practice.1 Japanese life expectancy is 86 years for women and 81 years for men. Along with the extension of life span, discrepancy between lifespan and healthy life causes problem due to huge expansion of medical cost.2 According to the Japanese government official, healthy life expectancy was 74.2 years for women, and 71.2 years for men, so it is nearly 12 years intervals for women and 10 years for men that needs any type of care to live.3 Here, healthy life is defined as not having activity limitation due to the health reason. Dietary control and physical activity are main factors to keep wellness and longevity but a combined method is still under developing.
Since ancient times, fasting has been performed for religious reasons or as a cure of diseases. Takahira4 was at the vanguard of fasting therapy in 1910-1920. He studied precisely the metabolic changes caused by fasting, and reviewed the efficacy of fasting therapy in various disease states. Mitsuo Koda5 developed fasting dietary therapy for various diseases, and confirmed beneficial effects for many patients with intractable diseases.
However, fasting method for healthy longevity or daily wellness has not been established. Our group had practiced macrobiotics for more than 10 years, and visited various fasting groups from 2005 to 2014.6 Upon these experiences we developed the teaching and practice system in 4-day “Wellness-fasting”. Daily nutritional intake was about 300 kcal by fermented vegetable juice (Ko-so). Many women had light headache in daily life, which became worse during fasting, but finally it disappeared, and substituted to vivid and active feeling to do something.
Our method could encourage participants to be a leader of health promotion by combining foods and health, and spiritual life. In this paper, we summarized the results of about 160 participants from October 2014 to December 2015.
METHODS
Subjects
About 20 healthy volunteers each time who wanted to learn wellness fasting by the ARSOA program. Data were collected from October 2014 to December 2015. Total number of participants in 12 courses was 161. Number of males was 36 and females 125. Age ranged from 20 to 74, averaging 46 years. Inclusion criteria to participate the program were healthy adults in any age in both sex, and exclusion criteria were diseased patients receiving drug therapy for cardiovascular disease, diabetes, chronic infectious diseases, gastrointestinal (GI) tract diseases, cancer and pregnant women
Persons who wanted to participate in the program were telephone-interviewed by the expert staff about their health and willing to the program. All participants were requested to send 1 week dietary records and health check sheet, including past history, abnormal laboratory data, habitual health foods and/or supplements, and any question to the counselor.
All participants signed the agreement sheet after precise explanation of the program.
The program had been approved by the Ethical Committee in the Life Science Promotion Association.
Program
The 4 day wellness fasting program is shown in Table 1. All participants gathered at the Relache Holistic Center in Megamino-mori, in Hokuto City, Yamanashi prefecture. For safety of the participants, nurses, athletics leaders, registered dietitians, and supportive staffs were joined in the study. For acute illness, near doctors in Suwa Central Hospital were contracted to treat sickness or unexpected accident.
Table 1: ARSOA wellness fasting schedule.
|
Hour
|
1st day
|
2nd day |
3rd day
|
4th day
|
|
5:00
|
|
Drink ko-so,
Respiration facing the rising sun |
Drink ko-so,
Respiration facing the rising sun
|
Drink ko-so,
Respiration facing the rising sun
|
|
7:00
|
|
Free time |
Free time
|
Free time
|
|
8:00
|
|
Health seminar
2. physical activity |
Health seminar
3. oil intake
|
Health seminar
4. diet after fasting
|
|
9:00
|
|
Macrobiotics |
Leader course
|
|
|
9:35
|
|
Drink time |
Drink time
|
|
|
10:00
|
|
Athletic program
1. walking to the rainbow farm |
Athletic program
2. walking to the shrine
|
Report writing and closing celemony
|
|
12:00
|
Registration |
Juice making by organic vegetables |
Vegetable juice
|
|
|
13:30
|
Health check-up |
Practice: hand healing |
Practice: hand healing
|
|
|
14:00
|
Stretch & walking in nature |
DVD “Forks over knives” |
DVD and discussion
|
|
|
16:00
|
Health Seminar
1. wellness fasting |
Lecture and Q&A |
|
|
|
17:00
|
Drink time |
Drink time |
Drink time
|
|
|
18:00
|
Writing on health check sheet |
Relaxation time |
Relaxation time
|
|
|
19:00
|
Adjourn (Hotel relache) |
Adjourn (Hotel relache) |
Adjourn (Hotel relache)
|
|
The participants registered at noon on the first day. After check-in, health check-up was done by the Body Composition Analyzer (Tanita, Tokyo, Japan) which measured body weight, fat volume, muscle volume, water contents, estimated bone weight, basal metabolic rate and body mass index (BMI), based upon the electric impedance. Blood pressure and pulse rate were measured by Omron HEM-7021 (Kyoto, Japan), and abdominal circumference was measured by a scale meter.
Each participant was requested to fulfill the health check-up sheet, including subjective psychological symptoms by 3 category (not feel, feel, strongly feel), such as headache, hungry, GI distress, nausea, fatigue, disgust or depression, general condition, vivid feeling, activity and skin condition.
After health check-up participants received the orientation for the fasting, stretch movement, walking, and relaxation. Next morning wake-up time was early to practice meditation toward the rising sun. Health check-up and intake of 50 ml fermented vegetable juice, ko-so, Cell Energy (multivitamins), and mineral tablets followed. After free time, 2 seminars for physical activity, and test for individual physical movement, including slow training and stretch were done.
On the 2nd day morning respiration and meditation facing to the rising sun or blue light were performed outside in early morning. Then, the seminar on diet, nutrition, cooking and health based upon the macrobiotics were carried out.
In the afternoon practice of hand healing was taught, and had discussion time about the food and health by seeing the DVD “Forks over knives”. At evening, relaxation stretch, selfmassage and meditation were practiced. In free time and night before sleep, participants could use foot spar, radon vapor bath, oil massage and walking in the nature around the hotel. As hotel facilities, foot bath, radon hormisis room and ordered massage were available in free time.
On the 3rd day, the schedule was repeated. Furthermore, music therapy and a field trip to the organic farm were carried out. Some vegetables harvested at the farm were used to make organic vegetable juice.
On the last day, attention to return to normal diet was taught, and the subjects ate half volume of boiled brown rice and vegetable soup as a brunch. All participants were requested to report their health condition after returning home (6th day and 1 month later).
Dietary intake during fasting: Each day, 2 litre bottle of water was recommended to drink. About 300 kcal was taken from 20- 50 ml concentrated fermented vegetable juice (Ko-so) drink 3 times a day (Table 2).
Table 2: Nutrients intake during fasting per day.
Ko-so contains 1.6 g galactooligosaccharide and has 1700 µM TE (AOU unit)
* DRI: Dietary Reference Intake 2010 for middle aged women.
|
Energy
|
Protein |
Lipid |
K |
Ca |
Mg |
Mn |
Zn |
Se |
Fe |
Vit A |
Vit D |
Vit B1 |
Vit B2 |
Vit B6 |
Vit C |
Dietry Fiber
|
|
kcal
|
g |
g
|
mg
|
mg |
mg |
mg |
mg |
µg |
mg |
mg |
µg |
mg |
mg |
mg |
mg |
g
|
|
Ko-so 150 ml
|
188 |
1.1 |
|
353
|
68 |
32 |
0.32 |
0.2 |
|
1.4 |
12 |
|
0.05 |
0.03 |
0.17 |
7 |
0.5
|
|
Mineral tab 5 tab
|
1.8 |
0.02 |
0.04
|
|
300 |
300 |
0.08 |
15 |
20 |
0.8 |
|
|
|
|
|
|
|
|
Cell-Energy 3 pack
|
72 |
0.6 |
0.3
|
66
|
124 |
8 |
0.3 |
0.02 |
|
0.3 |
|
57 |
6.6 |
4.5 |
9.2 |
300 |
4.2
|
|
Carrot juice 65 ml
|
65 |
0.8 |
0.3 |
355
|
30 |
13 |
|
0.3 |
|
0.3 |
721 |
|
0.08 |
0.06 |
0.82 |
28 |
3.6
|
|
Total
|
327 |
2.52 |
0.64 |
775
|
522 |
353 |
0.43 |
15.5 |
20 |
2.8 |
733 |
57 |
6.33 |
4.59 |
8.19 |
335 |
8.3
|
|
DRI*
|
1950 |
50
|
|
2000
|
600 |
290 |
|
|
|
6.5 |
700 |
|
1.1 |
1.2 |
1.1 |
100 |
17
|
Although intake of major nutrients were severely restricted, combination of Cell Energy (LIF origin, Japan) and Mineral (LIF orgin) provided enough vitamin and minerals compared to the Dietary Reference Intakes (DRI 2010). High antioxidant activity of Ko-so may give additional benefits for detoxication. In addition, a cup of warm soup made from dry mushroom and radish was supplied every evening before sleep. Hot water and tea were freely available.
Statistical Analysis
All data were collected in the excel database, and transferred to SPSS version 20 (IBM SPSS, Tokyo, Japan). Non-parametric variables, such as mood, were replaced to categorical variables. Significant level was set at p<0.05. We also used structural equation modeling (SEM) to examine presumptive underlying variables by AMOS version 19 for Windows (IBM Inc.). The analysis was performed using cross-lagged effects variation model with longitudinal data followed over one month. Estimation of the best fitting model was carried out by the method of maximum likelihood of SEM. Results were regarded as statistically significant if the p values was less than 0.05.>< 0.05. We also used structural equation modeling (SEM) to examine presumptive underlying variables by AMOS version 19 for Windows (IBM Inc.). The analysis was performed using cross-lagged effects variation model with longitudinal data followed over one month. Estimation of the best fitting model was carried out by the method of maximum likelihood of SEM. Results were regarded as statistically significant if the p values was less than 0.05.
RESULTS
The anthropometric data, blood pressure, pulse rate and body temperature are shown in Table 3. Age of participants ranged from 20 to 74, and most participants were women, who were working mostly in cosmetic shops as a sales lady or owners.
Table 3: Anthropometric data of participants.
|
Male (n=36)
|
Female (n=36) |
|
mean±sd |
mean±sd
|
|
Age (year)
|
43.4±8.3 |
46.9±13.0 |
| Height (cm) |
170.6±4.2 |
158.7±5.2
|
|
Body weight (kg)
|
67.1±8.5 |
55.3±8.5 |
| BMI (kg/m2) |
23.1±2.9 |
22.0±3.3
|
|
Fat percent (%)
|
21.1±4.9 |
31.1±6.0 |
| Muscular weight (kg) |
49.8±4.2 |
35.3±3.3
|
|
Systolic BP (mmHg)
|
129.1±15.1 |
123.3±20.9 |
| Diastolic BP (mmHg) |
85.3±12 |
91.9±13.0
|
|
Pulse rate (/min)
|
73.6±12.9 |
74.6±11.2 |
| Body temperature (°C) |
36.4±0.4 |
36.3±0.4
|
There were no current smokers. Their lifestyle was healthy and about half of them were ovo- and fish-vegetarians. BMI, blood pressure, body composition and body temperature were all within the normal range.
Changes of body weight, BMI, fat percent, blood pressure and pulse rate during 4 day wellness fasting is shown in Table 4. Body weight was lost 2.6 kg in males and 1.7 kg in females at median. Body fat rate decreased 1.3% and 0.7% in males and females, respectively, and muscular weight decreased 1.4 kg in males and 0.8 kg in females.
Table 4: Reduction of body weight, BMI, fat percentage, blood pressure and pulse rate during 4 days wellness fasting.
|
Males (n=31)
|
Females (n=111) |
| median |
(25.75 percentile) |
median |
(25.75 percentile)
|
|
Body weight (kg)
|
2.6 |
(1.9, 3.0) |
1.7 |
(1.4, 2.2)
|
|
BMI (kg/m2)
|
0.9 |
(0.7, 1.0) |
0.7 |
(0.6, 0.9)
|
|
Fat percent (%)
|
1.3 |
(0.1, 2.0) |
0.7 |
(-0.5, 2.0)
|
|
Muscular weight (kg)
|
1.4 |
(0.8,1.7) |
0.8 |
(0.2, 1.4)
|
|
Systolic BP (mmHg)
|
12 |
(3.5, 22.0) |
12 |
(5.3, 22.3)
|
|
Diastolic BP (mmHg)
|
5.0 |
(-1.3, 11.5) |
6.0 |
(‘0.0, 10.6)
|
|
Pulse rate (/min)
|
-10 |
(-17, 2.0) |
-7.5 |
-15, 2.0)
|
|
Body temperature (°C)
|
0.2 |
-0.1, 0.4) |
0.3 |
(0.3, 0.8)
|
Systolic blood pressure decreased 12 mmHg in both males and females, and 5 mmHg and 6 mmHg in diastolic pressure in males and females, respectively. On the contrary, the pulse rate increased 10 in males and 7.5 in females at median. Body temperature decreased 0.2-0.3 o C in both sex.
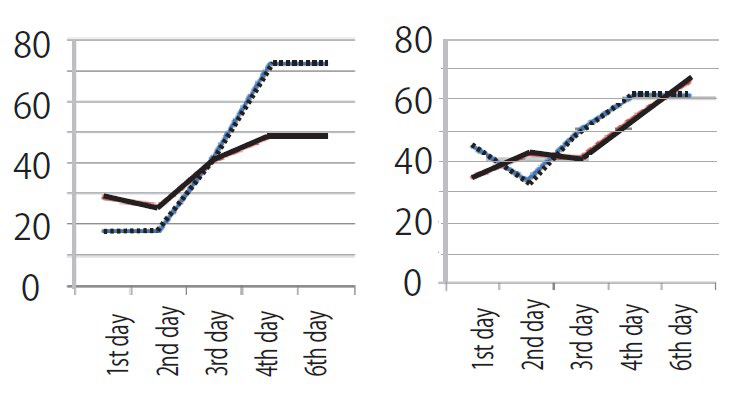
Changes of self-reported condition during 4 days are shown in figures (Figures 1 and 2). Slight headache was a complaint of about one third women, and the prevalence increased toward 3rd day, but it decreased thereafter to only 10% in females. Hungry was highly recognized among males, but high prevalence was only 2 days. Feeling of coldness was common complaint of women, and it improved only 15%. GI tract distress was rather stationary around 20%. Vivid feeling and activity increased toward the end of fasting. In males increase of vivid feeling was remarkable at day 4 and day 6. Active feeling and vivid mood were significantly associated with skin condition.
Figure 1: Prevalence of headache (upper left), Feeling of Hungry (upper right), Prevalence of GI distress (lower left), and Cold feeling (lower right). Solid line: female, dot line: male. Vertical axis; prevalence rate (%).
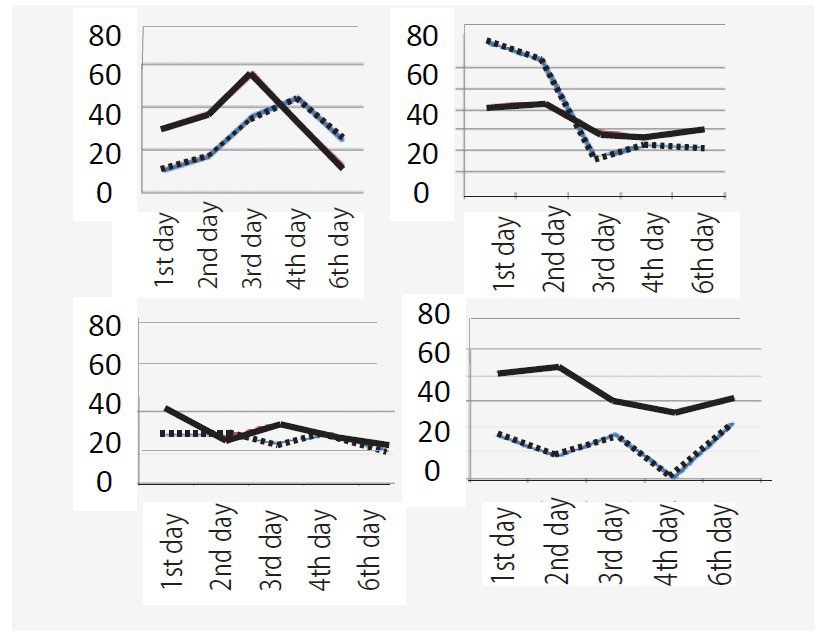
Figure 2: Prevalence rate of good condition (left) and feeling of activities (right) Vertical axis; prevalence rate (%).
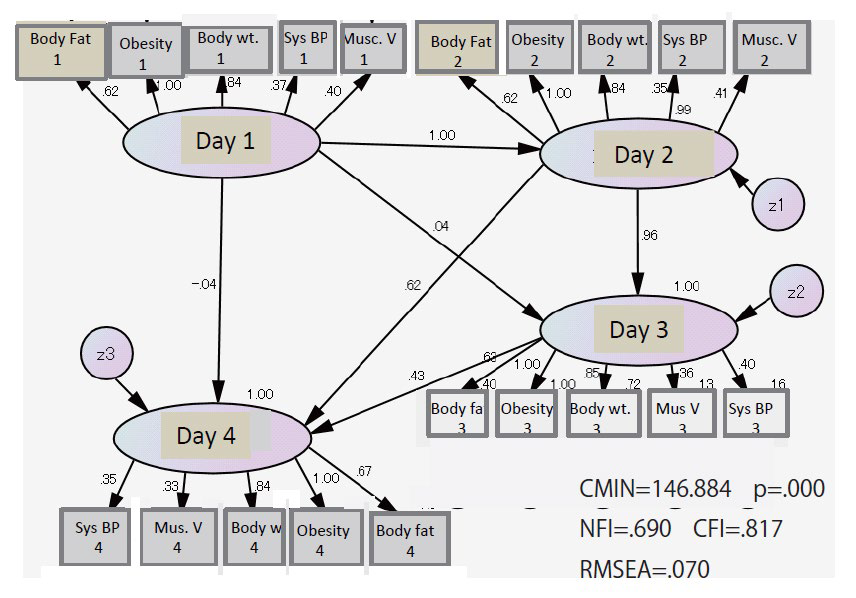
Hungry, GI distress and feeling of emesis were significantly associated with fat, muscle weight reduction and decreased BMI. General condition, sleepy feeling, fatigue, depressive feeling, headache, cold feeling, GI distress and hunger were varyingly interrelated. Structure Equation Model by AMOS showed that a significant multiple effects of body fat rate, obesity, body weight, muscle volume and systolic blood pressure at day 2 and day 3 was recognized to those at day 4 (Figure 3).
Figure 3: Causal structure of objective physical health by using structural equation modeling. Physical health of day 4 is influenced by day 2 and day 3.
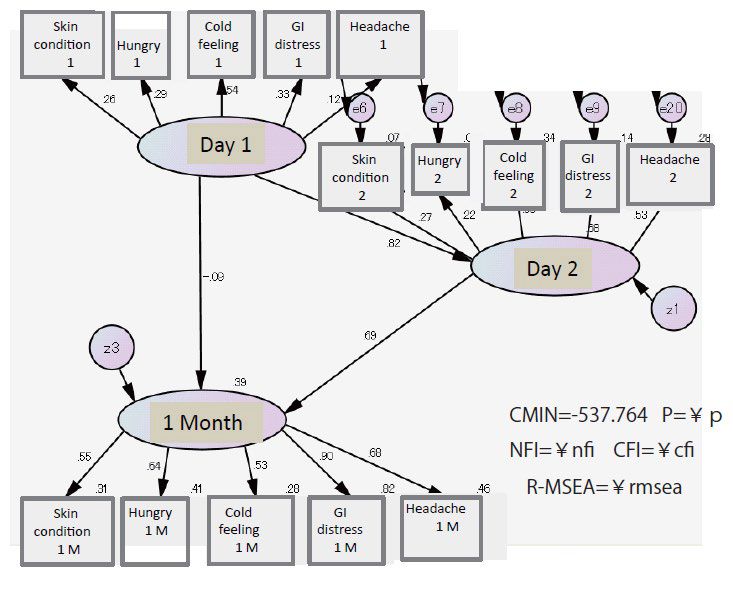
Subject symptoms, such as skin condition, hungry, cold feeling, GI distress and headache 1 month later was significantly influenced by those of day 2 (Figure 4).
Figure 4: Causal structure of subjective health by using structural equation modeling. About 60% of subjective health 1 month later could be explained by the conditions on day 2.
Symptoms, mood and body changes interacted and became better in later days.
DISCUSSION
In 1999, during the International Year of Older Persons, World Health Organization (WHO) launched a new campaign highlighting the benefits of Active Ageing.7 This was in perfect harmony with the slogan for the International Year “Towards a Society or All Ages” as Active Ageing highlights the importance of social integration and health throughout the life course. Dr. GroHarlem Brundtland, Director General of WHO stated “there is much the individual can do to remain active and healthy in later life”. The right life style, involvement in family and society and a supportive environment for older age all preserve well being.
It is important to make strategies required at the services delivery level and possible tools for implementation. Integrated organization by various health providers, such as physicians, nurses, dieticians, physical exercise trainers, pharmacists, therapists, and others, work together putting people at the center.3 It should be important to set standards for team-based care through multidisciplinary learning based upon the theoretical and practical learning.
In response to increasing rates of obesity and associated chronic disease, Japan has implemented several policies, guidelines and programs. Kenkou Nippon 21 (Health Japan 21) began in 2000,9 followed by the Shokuiku (food and nutrition education) Basic Law which was passed in 2005.10,11 Subsequently, in 2008, the government launched a special health check-up (tokutei kenkou shinsa), involving measurement of waist circumference and nutrition counseling to reduce metabolic syndrome.12
However, despite of these programs and guidelines, obesity remains a public health problem in Japan. In addition, discrepancy between lifespan and healthy life expectancy causes another problem by huge expansion of medical cost.13 The difference was nearly 12 years for women and 10 years for men, and it is not shrunken despite of the implementation of various health strategies for elderly care.
Various dietary therapies to control health and body weight have been proposed, such as macrobiotics, Atkins diet, Zone diet, Ornish Diet, Learn Diet, etc.14 We had supported basically Macrobiotics,6 and elaborated to take the balance of food, physical activity and mind to achieve a spiritual life. It is relevant of the Koda’s fasting therapy,5 in which unpolished brown rice and green vegetable paste constitute the basic regimen, and it improves the intestinal environment by resolving constipation. Koda’s method could repair the balance of autonomic nervous system, so it may not only be effective for gastrointestinal disease, but also for some neurodegenerative diseases.
Although control of total energy intake is essential to control obesity, individual awareness and practice are also important.14 We developed a weight loss program based on a behavioral approach with dietary and exercise intervention (Saku Control Obesity Program (SCOP)) in Japan.15,16,17 In this program, we emphasized individually-tailored counseling, instead of uniform class room teaching, and the diet and physical activity were designed for each participant.18,19,20 Half participants succeeded to reduced more than 5% body weight, and to change to the good lifestyle.
In ARSOA Wellness Fasting method is the combination of a low-energy vegetarian diet (about 300 kcal fermented vegetable juice per day, and multivitamin and mineral supplement), physical exercise (walking, slow training and stretch), meditation, foot spar, radon hormisis, and self massage with/without oil to stimulate the self-healing capacity. Using this regimen, a new concept of fasting for healthy longevity would be established.
The changes of mood were related to the body change. Headache was the most popular symptom, as one 3rd female participants had slight headache at registry, but it remarkably improved after fasting. Hungry and GI distress, nausea appeared on the second and 3rd day, but these improved toward the end. Blood pressure and fat percent significantly decreased by fasting, and body temperature tended to become lower. The active and vivid feeling increased on fourth day, and it lasted even at one month later.
It has been shown that a few days fasting caused many metabolic changes including various hormones and free fatty acid.21 The altered metabolism by fasting needs further study, because fasting seems to cause switch fuel from carbohydrate to fatty acid, as shown by the increase of ketone bodies in the urine.22 Cahill23 studied metabolic changes during 40 days of starvation and found that β-hydroxybutyrate replaces glucose as a source of energy. Fasting causes many metabolic changes.24
We suggested the contribution of intestinal microbiota was also important.25 We considered the increased β-hydroxybutyrate should influence on both mental and somatic symptoms. Butyrate made by intestinal microbiota could be metabolized to β-hydroxybutyrate in the body, so these should be further studied in the near future.
ACKNOWLEDGEMENTS
The authors thank to participants and many staffs of wellness fasting for their cooperation. The study was supported by the ARSOA Educational Program.
CONFLICTS OF INTEREST
The authors declare that they have no conflicts of interest.


