INTRODUCTION
Task shifting refers to the rational redistribution of tasks from health professionals to community health workers in order to improve access to care and optimize the use of limited human resources. Since 2006, global attention has been drawn towards human resources for health crisis, which is worse in lower income countries.1 This crisis has re-energized the focus on the use of community health workers in service delivery, through task shifting. Task shifting has gained in prominence and urgency to meet the demands concerning the health systems.2,3,4,5
The primary healthcare strategy adopted by the World Health Organization (WHO) at Alma-Ata6 promoted the initiation and rapid expansion of community health volunteer (CHVs) programs in low and middle income country (LMIC) settings in the 1970s.7 However, researchers questioned the effectiveness and cost of such programs in the following decade, particularly due to high attrition rates that tend to push up the cost of training. Thus, although volunteering constitutes an essential aspect of primary healthcare, being able to identify and allocate health tasks preferred by volunteers would improve the efficiency of such programs.
Existing studies demonstrate that CHVs play a critical role in providing household services, substituting for health professionals participating in a range of tasks,1,8,9,10 in the quest towards universal health coverage and sustainable development goals.4,11,12,13,14,15,16 CHVs help increase access to, and facilitate the use of healthcare services during medical cases as tuberculosis, immunization and family planning programs, particularly in populations with limited access to healthcare facilities.17 In complying with the expectations and having received sufficient investment and support, community health workers (CHWs) show great potential towards strengthening the current situation of health systems.18 Yet such task shifting to volunteers should be carefully done to ensure that the secured livelihoods of the volunteers themselves are not compromised in the process. Kaseje and Sempebwa19 argued that CHV programs fail because of unrealistic expectations, irrational allocation of tasks, poor planning and an underestimation of the effort and input required to work with CHVs. Assignment of tasks may not always be in the interest of volunteers, thus, arising the need to gain an understanding of the tasks they prefer. This is necessary for a meaningful and sustainable task shifting to volunteers.
Despite its importance, surprisingly, little research has examined as to how volunteer motives relate to their task preferences in the African setting. Studies provide clues that volunteers’ experiences are likely to be an important determinant for sustained involvement in volunteering, but there is inadequate information to explain the factors that shape these experiences. Only a handful of studies have examined sustained participation, which is typically measured in terms of the number of hours that volunteers are willing to work and for what period of time. Snyder et al20 suggested that there may be variations in tasks suitable for different volunteers. Specifically, how task preference relates to volunteer motives in African settings have not been investigated. While many studies have demonstrated the effectiveness of CHVs4,14,18 and led to the understanding that it is a more cost-effective approach to implement their participation to complement for the available formal services towards saving lives than the formal healthcare system working without their involvement.21 The aim of this study was to investigate the relationship between volunteer motives and their task preference. The specific objective was to determine the relationship between volunteer motives and their task preference in an African setting.
METHODOLOGY
The study adopted a cross-sectional design comparing task preference among long serving volunteers and non-volunteers as well as examining relationship with volunteer motives. Five hundred and thirty-one CHVs in Nyakach, Rarieda and Butere Sub-Counties, West Kenya who had served for five years or more, were included in the study. For each CHV participating in the study, their nearest next door neighbor of the same sex, education and age group, was included resulting in a sample population 1062 respondents. The eight motives (altruistic, materialistic, development of understanding, career development, esteem, social and spiritual) were introduced from phase 1 of the study22 while the tasks were derived from the common health activities undertaken by volunteers in Kenya. Data collection was performed using self-administered questionnaires to be filled by the participants under the supervision of the researcher and research assistants. The preference of the respondents for each of the tasks was recorded on a 1-5 Likert scale. Comparative analysis was undertaken for assessing the task preference among volunteers on the basis of motives and volunteer status.
The questionnaire was based on a volunteer assessment framework with eight motive constructs developed by Ochieng B.M and her colleagues.22 The respondents were gathered at one center in each of the sub-counties for them to fill out the questionnaires. The tool presented the participants with descriptions of 13 common Kenyan health volunteer tasks and asked them to rank the tasks in the order of their preference for performing them, indicating the “most preferred choice” and “least preferred choice.” Their level of preference in performing each of the tasks was then measured on a 1-5 Likert scale.
Data Analysis
The data was analyzed using Scientific Package for Social Sciences (SPSS® version 16) computer package to describe the outcome variables for each of the study groups. The comparative analysis was performed for cases and controls, where the comparison was centered on the association between motives and task preference. Bi-variate descriptive analysis was undertaken to compare the relationship of motives for volunteering to task preference between the cases and the controls.
The comparative pooled analysis method was used to compare the association of motives with tasks preferred among volunteers. A Poisson regression model was used to assess the effect of volunteer motives on task preference. The Poisson regression model was used because the outcome of interest was considered as count data and the data was analyzed on a population level. The study also used mean scores to compare between volunteers and non-volunteers by the use of pooling of “means”.
RESULTS
Socio-Demographic Characteristics
The targeted respondents filled the questionnaires yielding a 100% response rate. The majority of the respondents were female 648 (59%), equally distributed between the volunteers and non-volunteers. A majority of the respondents were aged between 36 to 50 years. Almost all the respondents had a good level of education with almost 540 (50.8%) having completed primary education and 510 (48.2%) having finished secondary level of education. The respondents were evenly distributed geographically as has been reported in Table 1.
| Table 1: Distribution of Sample Population by Age, Sex, Education and Residence. |
|
Nyakach |
Rarieda |
Butere |
Total |
|
Volunteer |
Control |
Volunteer |
Control |
Volunteer |
Control |
|
| Age |
n (%) |
n (%) |
n (%) |
n (%) |
n (%) |
n (%) |
N (%) |
| 20-35 |
49 (27.7) |
49 (27.7) |
32 (18.1) |
32 (18.1) |
42 (23.7) |
42 (23.7) |
246 (23.2) |
| 36-50 |
121 (68.4) |
121 (68.4) |
125 (70.6) |
125 (70.6) |
107 (60.5) |
107 (60.5) |
706 (66.5) |
| >50 |
7 (0.4) |
7 (0.4) |
20 (11.3) |
20 (11.3) |
28 (15.8) |
28 (15.8) |
110 (10.4) |
| Total |
177 (96.5) |
177 (96.5) |
177 (100) |
177 (100) |
177 (100) |
177 (100) |
1062 (100) |
| Sex |
n (%) |
n (%) |
n (%) |
n (%) |
n (%) |
n (%) |
N (%) |
| Male |
86 (44.1) |
86 (44.1) |
70 (39.5) |
70 (39.5) |
69 (39) |
69 (39) |
450 (41) |
| Female |
109 (55.9) |
109 (55.9) |
107 (60.5) |
107 (60.5) |
108 (61) |
108 (61) |
648 (59) |
| Total |
195 (100) |
195 (100) |
177 (100) |
177 (100) |
177 (100) |
177 (100) |
1098 (100) |
| Educ. |
n (%) |
n (%) |
n (%) |
n (%) |
n (%) |
n (%) |
N (%) |
| None |
|
7 (0.4) |
|
|
3 (.2) |
2 (.1) |
12 (0.01) |
| Prim. |
104 (58.8) |
100 (56.5) |
72 (40.7) |
76 (42.9) |
92 (52) |
96 (52) |
540 (50.8) |
| Sec. |
73 (41.2) |
70 (39.5) |
105 (59.3) |
101 (57.1) |
82 (46.3) |
79 (44.6) |
510 (48.2) |
| Total |
177 (100) |
177 (96.4) |
177 (100) |
177 (100) |
177 (98.5) |
177 (96.7) |
1062 (100) |
Although, a majority of the non-volunteers showed a limited experience in the volunteers’ service, a third (31.5%) of them had a volunteering experience of over 1-5 years. Two thirds of the volunteer population had prior experience of over five years with a large proportion, nearly 40%, having more than ten years of experience (Table 2).
| Table 2: Length of Voluntary Service by Volunteer Status. |
| Length of service |
|
Volunteers |
Non-Volunteers |
Totals |
| <1 year |
0 (0%) |
354 (67%) |
354 (33%) |
| 1-5 years |
201 (38%) |
164 (31.5%) |
365 (34%) |
| 6 to 10 years |
122 (23%) |
6 (1%) |
128 (24%) |
| >10 years |
208 (39%) |
7 (1%) |
215 (20%) |
| Total |
531 (100%) |
531 (100%) |
1062 (100%) |
Association of Task Preference to Long Serving Volunteers
Comparing the mean scores of task preference by volunteers and non-volunteers, the findings showed that the level of preference for tasks described was statistically significantly higher among volunteers than non-volunteers (p=0.00) except for emergencies and community surveys, where the difference was minimal (Figure 1). The results identified two categories of tasks: first, the long-term tasks that were strongly preferred by the long serving health volunteers than non-volunteers. These were typical health tasks such as maternal child health, tuberculosis/human immunodeficiency virus (TB/HIV) defaulter tracing, identification and referral of people with chronic cough and provision of curative services (Figure 1).
Figure 1: Mean Scores of Task Preference by Cases and Control
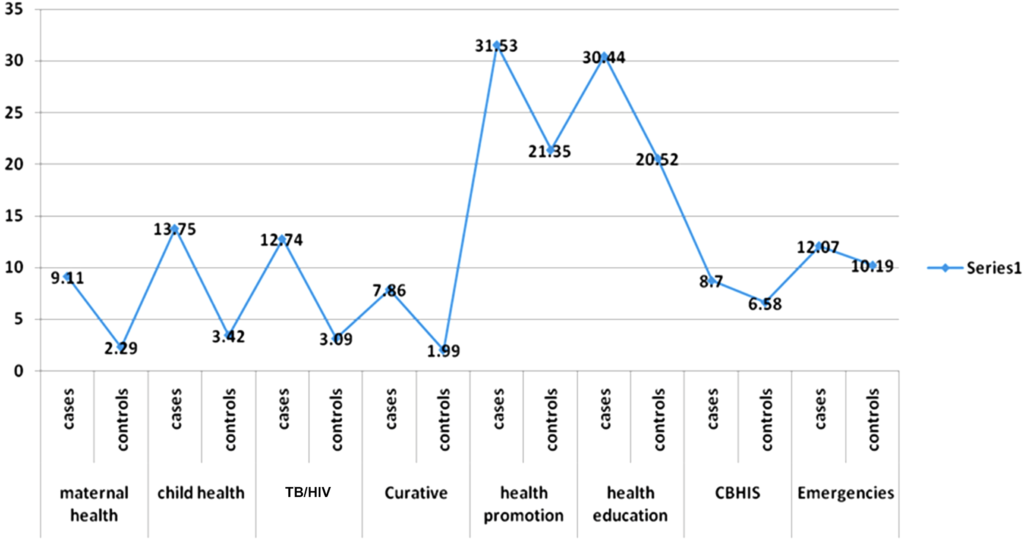
The second category included long-term tasks such as community household surveys, and attending community dialogue meetings, and short-term emergency tasks that were preferred equally by all the participants, both volunteers and non-volunteers. The proportion of respondents preferring the short-term tasks was not statistically significantly higher among volunteers than non-volunteers (Figure 1). The tasks that were either short-term or of an emergency nature, required an urgent response for relatively short periods such as campaigns, spraying of houses with insecticides to protect them from malaria, disaster and emergency response to floods, famine and disease outbreaks. These were tasks that demanded urgent participation of the volunteers and non-volunteers. Though preferred slightly more by volunteers, non-volunteers expressed substantial preference as well (Figure 1).
Association of Task Preference to Volunteer Motive Constructs
Comparing mean scores of task preference by core motive constructs, altruistic and self-seeking, the findings of the study showed that the level of preference of tasks described was statistically significantly higher among participants with altruistic than those with material gain motives except for emergency tasks, where the difference was minimal (Figure 1). We tested the association of tasks with core motives using the Chi-square test. The long-term health tasks such as maternal child health, TB/HIV defaulter tracing, identification and referral of people with chronic cough (Table 3) were strongly preferred more by people with altruistic than self-seeking motives. Non-health long-term tasks such as community household surveys and attending community dialogue meetings, were almost similar to short-term emergency tasks in that they were preferred equally by all the study participants, (volunteers and non-volunteers) irrespective of their motives (Table 3). The tasks that were either short-term or of an emergency nature, demanded response for relatively shorter periods such as in campaigns, spraying of houses with insecticides to protect them from malaria, disaster and emergency response to floods, and disease outbreaks, though preferred slightly more by people with altruistic motives, those with self-seeking motives showed substantial preference as well (Table 3).
| Table 3: Association of Volunteer Tasks with Core Motive Constructs. |
|
Altruistic Motive |
Material gain Motive |
| Volunteer Tasks |
B (co-efficient determinant) |
p Value |
B (co-efficient determinant) |
p value |
| Maternal Health |
0.061 |
0.00 |
-0.033 |
0.07 |
| Child Health |
0.087 |
0.00 |
-0.048 |
0.08 |
| Curative Care |
0.044 |
0.00 |
0.007 |
0.73 |
| TB/HIV care |
0.063 |
0.00 |
-0.045 |
0.13 |
| Home visits for HE |
0.123 |
0.00 |
0.000 |
0.99 |
| Family Planning |
0.016 |
0.13 |
0.012 |
0.39 |
| Care of OVCs |
0.017 |
0.01 |
0.000 |
0.98 |
| Meetings/Dialogues |
0.013 |
0.00 |
-0.004 |
0.53 |
| Campaigns |
0.011 |
0.92 |
-0.013 |
0.11 |
| Disaster activities |
0.025 |
0.00 |
-5.320 |
0.99 |
| Out Breaks |
0.017 |
0.02 |
0.021 |
0.12 |
| Emergencies |
0.056 |
0.01 |
0.02 |
0.37 |
Findings of the study showed that most of the tasks such as maternal health, child health, curative care, home visits for health education, TB/HIV defaulter tracing, taking care of orphans and vulnerable children, holding dialogue meetings with community members, helping in disasters, emergencies and outbreaks were significantly associated with altruistic values more than material gain motives (p=0.00). The only tasks that were not significantly associated with altruistic than material gain motives were family planning and immunization campaigns (p=0.92) (Table 3). Emergency tasks were preferred by all motives categories. Tasks did not demonstrate a clear pattern of relationship with the additional motive constructs beyond altruistic and material gain.
The non-core motive constructs did not demonstrate consistent association with task preference; however, we note that, spirituality demonstrated a relationship with the largest number of tasks: home-visits for health education, disasters and emergencies (Table 4).
| Table 4: Association of Volunteer Tasks with Additional Volunteer Motives. |
|
Development of understanding |
Career Development. |
Esteem |
Social |
Spiritual |
| Volunteer tasks |
B (co-efficient determinant) |
p value |
B (co-efficient determinant) |
p value |
B (co-efficient determinant) |
p value |
B (co-efficient determinant) |
p value |
B (co-efficient determinant) |
p value |
| Maternal health |
0.000 |
0.95 |
0.008 |
0.77 |
-0.020 |
0.43 |
-0.023 |
0.32 |
0.015 |
0.57 |
| Child health |
-0.004 |
0.97 |
0.017 |
0.66 |
-0.041 |
0.26 |
-0.034 |
0.32 |
0.016 |
0.68 |
| Curative care |
0.018 |
0.33 |
-0.030 |
0.33 |
-0.040 |
0.17 |
0.018 |
0.50 |
0.023 |
0.46 |
| TB/HIV care |
0.035 |
0.17 |
-0.006 |
0.89 |
-0.046 |
0.24 |
-0.038 |
0.29 |
0.45 |
0.27 |
| Home visits for HE |
0.041 |
0.35 |
0.028 |
0.70 |
-0.080 |
0.23 |
0.035 |
0.57 |
0.161 |
0.02 |
| Family planning |
0.002 |
0.89 |
0.003 |
0.88 |
-0.029 |
0.12 |
0.032 |
0.06 |
0.013 |
0.50 |
| Care of OVCs |
0.011 |
0.17 |
-0.030 |
0.02 |
0.013 |
0.30 |
0.008 |
0.48 |
0.009 |
0.51 |
| Meetings/dialogues |
0.004 |
0.43 |
0.014 |
0.11 |
-0.015 |
0.06 |
0.014 |
0.06 |
0.011 |
0.20 |
| Campaigns |
0.023 |
0.00 |
-0.004 |
0.73 |
-0.011 |
0.32 |
0.016 |
0.13 |
0.001 |
0.93 |
| Disaster activities |
0.001 |
0.09 |
-0.012 |
0.45 |
0.003 |
0.84 |
-0.008 |
0.54 |
0.050 |
0.00 |
| Out breaks |
0.005 |
0.54 |
-0.013 |
0.34 |
0.008 |
0.54 |
0.000 |
0.98 |
0.021 |
0.12 |
| Emergencies |
0.015 |
0.55 |
-0.029 |
0.49 |
-0.014 |
0.71 |
-0.014 |
0.70 |
0.117 |
0.00 |
Development of understanding demonstrated a relationship only with campaigns; career enhancement, only with the care of orphans and vulnerable children, and the social constructs (esteem enhancement and social adjustment) demonstrated a weak relationship with meetings and dialogues (Table 4). Altruistic motive constructs were associated with the largest number of tasks, followed by esteem enhancement motive. Curative care task was associated with the largest number of motives followed by emergency tasks (Table 3). The less preferred tasks were family planning and community-based health information system.
DISCUSSION
This paper presents an assessment framework that can be used to identify CHVs according to their task preference, for use in recruitment and deployment of volunteers and thus improve the cost-efficiency of the programs. The task preferences associated with volunteer motives were identified. The results seemed to suggest that task preference was most consistently associated with the two core volunteer motives (altruistic value and material gain) described by Ochieng and colleagues.22 The results indicated that altruistic motive was the reason behind volunteering with over 80% of the volunteers preferring 11 out of the 12 tasks (Table 4). The rest of the motives related inconsistently with task preference. Thus, the study identified the same core motives and how they could be applied for the classification of tasks to help categorize and deploy CHVs for efficient task shifting. Using the existing framework, individuals could be matched to the tasks they were likely to find most rewarding and thus help promote retention among the CHVs.
Individuals with altruistic motives preferred all tasks whether long-term or short-term. Whereas, individuals with material gain motives tended to prefer short-term emergency tasks. It is important that they are identified at recruitment so that they are not assigned and trained for long-term health tasks since they are likely to drop out. Task preference for all the 13 health tasks examined was higher among the known long serving volunteers than non-volunteers.
Finkelstein in 2008 reported a positive correlation between time spent in volunteering and motives.23 This observation is consistent with the finding in this study that all long-term health tasks requiring considerable investment of time were preferred significantly more by known volunteers than non-volunteers. Penner and Finkelstein24 also found that altruistic motives predicted the amount of time individuals spent in volunteering. These findings provided a basis for linking the motives to task categories. According to functional analysis,25,26,27,28 people volunteer in order to satisfy one or more needs or motives that relate to task categories.
The tool developed by Ochieng and colleagues22 provides a method for describing the CHVs tasks and ranking them in the order of their preference. The functional approach underlies the importance of matching volunteer motivations to the benefits that volunteerism provides. Clary et al26 found that undergraduate students with matching benefits were more satisfied with their volunteering experience and had greater intentions to continue volunteering. Hence, the importance of considering task preference in task allocation was elucidated. Furthermore, when given a choice, individuals preferred tasks with benefits that matched their personally relevant motives. Houle et al29 found that individuals chose volunteer tasks that they perceived would satisfy the motives that were most important to them.
Thus, individuals who satisfied altruistic tests were the best suited for recruitment and training as CHVs. They could be deployed for implementation of intervention programs to reduce child mortality, such as neonatal care and promotion of exclusive breastfeeding30 recognition and treatment with antibiotics of sick newborns,7 as curative care was among the tasks preferred in this study. Delivery of interventions in the home by CHWs was viewed as a critical aspect31 and visiting homes was identified among the preferred tasks in this study. Maternal care was strongly preferred by long serving volunteers. Syed and colleagues found that CHVs were effective in tracking pregnant women through the postnatal period and in raising awareness about appropriate maternal and newborn care practices.32 This, in turn, required greater investment towards programs for CHV selection and training.
Researchers assert that a favorable evaluation of an experience is a robust and reliable predictor of repeated engagement in that experience.33 This study added the dimension of identification and use of motives to predetermine their task preferences and therefore the need for training. This would improve the efficiency of the program by targeting training in content and length according to the realistic expectations of workers according to the categories defined in this paper. In this way long serving volunteers could be identified at recruitment for training, targeting preferred tasks.
Home visiting for health education, was among the most critical tasks for volunteers. It was associated with more than five motives. CHVs thus play an important role in helping to achieve the universal health coverage and sustainable development goals reported by many researchers.4,11,12,13,14,15,16 To these would be added emergency and data management tasks, focusing on volunteers with altruistic values. Finkelstein, and his co-workers demonstrated that the fulfillment of motives was a good predictor of volunteer tasks and longevity.20,23,35
One chief characteristic of volunteerism in community health was that it needed to be sustained, long-term. This study demonstrated that it may be possible to classify tasks according to the motives they satisfy. Other workers have reported that when volunteering met the motives for helping, individuals reported greater satisfaction in volunteering.25,26,36 This study added to the specific categories relevant to the health volunteers: long-term health, and developmental and short-term tasks required in disasters and emergencies.
If the managers of volunteer programs develop a list of tasks in the implementation of activities at the community level, that satisfy various motives suggested in this paper, they would be able to recruit from a larger pool of individuals, the appropriate volunteers. Volunteer recruits would be better able to find tasks with benefits that match their personal motives resulting in higher satisfaction and commitment to serve their communities. As shown in these studies, people prefer tasks they think will satisfy motives important to them.24,35,37
The view expressed by the findings of Houle, Sagarin, and Kaplan29 found that “people do differentiate tasks based on the volunteer motives they satisfy”. A task can be classified in terms of the motive(s) it does or does not satisfy. The results from this study were based on this idea and offered a classification of tasks. Further, psychological and sociological research suggested that experiences encountered while volunteering were the primary determinants of whether people decided to continue volunteering and hence the tasks that community volunteers preferred to undertake.27,38,39
CONCLUSION
The study concluded that the volunteer assessment framework developed by Ochieng and her colleagues is useful, not only in the identification of volunteers likely to volunteer long-term but also in the assignment of tasks they are likely to prefer and that would satisfy their motives for volunteering. It is noteworthy that the two constructs, altruistic value and material gain are adequate, both to identify long-term volunteers and to allocate them the most appropriate tasks. This would contribute to sustainability of volunteer initiatives.
The study demonstrated that it is possible to classify tasks according to the motives they satisfy. The results suggest that maternal child health, curative care, household visits lie in one class; community health surveys, and community meetings are within another and emergency tasks are in a third cluster. This will help volunteer recruiters to align them to tasks with benefits that match their personal motives resulting in higher satisfaction and commitment to serve their community for long. The proposed volunteer assessment framework (VAF) can thus be used to align volunteers to tasks, short-term (emergency), and long-term as CHVs.
COMPETING INTERESTS
The authors declare no competing interests.


