INTRODUCTION
The global mental health treatment gap is enormous and represents a gross inequity that exists with people’s ability to access mental health provisions in low-income and middle-income countries (LMICs).1 The World Health Organisation (WHO) shows that the global burden of mental disorders is increasing and predict health systems throughout the world will not be able to cope.2 Approximately, 85% of the world population reside in 153 LMICs and more than 80% of people who have a mental disorder are located within these LMICs.3 However, approximately 90-95% of mental health resources, including human resources for psychological therapies are being delivered in countries that only account for 5% of the population.4,5,6,7,8 This is a global inequity and it is unjust.1
It has been estimated that 50% of all lifetime cases of mental health begin by age 14 and 75% by age 24.9 Mental health disorders are estimated to affect 10-20% of youth in LMICs.10 This conservative estimate fails to address issues related to demand side barriers, inhibited by factors such as stigma, or supply side barriers.11,12 This may be related to a higher number of stress related trigger events such as natural disasters, war and conflict or poverty.13
In Bangladesh, over 6 million people experience depressive disorders and almost 7 million people have anxiety disorders.14 It is estimated that more than 10,000 people are dying by suicide in the country.15 Among students aged 13-17 in Bangladesh, 4% of boys and 6% of girls consider attempting suicide.16 In the Bangladesh National Survey (2019) it was accepted that at least 14% of children between 7-17-years suffer from mental health issues and yet 94.5% do not seek medical attention.17
Mental health stigmatization can prevent seeking help and worsen youth mental health.18,19 The National Institute for Health and Care Excellence (NICE) guidelines,20 have provided evidence that awareness programmes can facilitate support for youth with mental health issues. Emphasis is put on the dissemination of mental health literacy being filtered down from service providers and support networks, to communities to enable them to effectively provide evidence-based psychosocial interventions for young people.18,19,20 Psychosocial interventions are likely to be important in young people for promoting resilience and reducing the prevalence of mental health disorders.19
This current research was designed to explore the understanding of mental health from the perspectives of teachers, parents, and students, from two schools in Bangladesh, one in a rural location and one within Dhaka, the capital city of Bangladesh. Our mixed methods approach embraces action-research using an evidence-based approach so the impact of solutions will be within months as opposed to years or decades. This paper represents the first stage in this approach, which is divided into two parts: 1) the assessment of student needs and 2) the exploration of beliefs and attitudes by parents and teachers regarding their understanding of mental health.
MATERIALS AND METHODS
All respondents were briefed that the aim of the research was to investigate ‘how to help students in school’. Schools pre-selected students who they believe would benefit from possible future intervention, either due to a mental health issue or with a learning difficulty problem of some kind. No description of mental health was given as a primary objective of the study was to investigate the understanding of ‘mental health’ from the perspective of the student, parent and teacher between the rural and the city location. Other than the administration of questionnaire and interviews, no additional material was given to any of the respondents. No clarification was provided on what the term mental health means during this stage of the investigation. This ongoing study protocol was approved by departmental Research Ethics Committee.
The original protocol involved an additional recruitment strategy designed to reach a greater number of respondents to enable the use of parametric statistics. However, the preliminary data obtained was cut short due to coronavirus disease 2019 (COVID-19) outbreak, resulting in early collation of data. The numbers reached were considered sufficient to carry out non-parametric statistical analysis.
The Strength and Difficulties Questionnaire
SDQs were sent to 40 teachers, 40 students and 40 parents, with a 50:50 split between rural and city locations and between male and female students (52% male and 48% female). However, the response rate regarding the completion of the SDQs was as follows: student respondents (n=23; rural n=17 and city n=6), parent respondents (n=18; rural n= 12 and city n=6) and teacher respondents (n=22; rural=16 and city n=6). All student respondents were between 7 and 14-years of age. The SDQ was available to all respondents in English as well as a professionally translated copy in Bengali. For access purposes, should a respondent be unable to read or write in either English or Bengali, the questions were read out to the respondent by the field researcher, who was fluent in English and Bengali, and answers described when required.
The self-reporting form of the SDQ is a standardised measurement instrument widely used for the assessment of different emotional and behavioural problems related to mental health in children and adolescents.20 The SDQ is made up of a total of 25 statements distributed across five scales: Emotional symptoms, conduct problems, hyperactivity, peer problems, and prosocial behaviour. With the exclusion of prosocial behaviour, all total scores accumulated results in the total difficulties score of the SDQ, which ranges from 0-40. The higher scores representing a poorer mental health.21 Scores between 0-13 are considered within the ‘normal’ band, 14-16 is the ‘borderline’ band and above 17 is within the ‘abnormal band’.
Significant differences were identified using the standard Mann–Whitney U tests for comparisons between two groups, p<0.017 was considered statistically significant. Tests of the three a priori hypotheses, that significant differences would be observed between rural and city locations within the teacher, student and parent subpopulations, were conducted using Bonferroni correction adjusted alpha levels of 0.017 per test (0.05/3). In addition to this, descriptive statistics were applied.
An accepted quantitative methodological limitation within this study is a lack of a control group. Therefore, total difficulties scores should be viewed with some element of caution.3
Semi-Structured Questionnaire
Due to time restrictions presented by the outbreak of COVID-19, Teachers were asked to complete a semi-structured questionnaire in leu of a semi-structured interview. This included a SDQ component as well as open-ended questions that explored the concept of mental health. This included requesting a definition of mental health and asked teachers if they have witnessed any risk-taking behaviours, such as self-harming, drug or alcohol use, violent or aggressive behaviours to others, etc.
Semi-Structured Interview
Students and parents undertook a semi-structured interview, designed to explore their understanding of mental health and to assess the needs of individual student’s. Questions explored access to education, educational histories, aspirations, responsibilities that impact attendance, stressful events, family dynamics and any known learning difficulties. Questions were asked to explore the symptomology and behaviour associated with mental health disorders, such as hallucinations, delusions, confusion, disturbed thoughts, obsessions, compulsions, depression, emotion regulation, anxieties, eating, sleeping patterns and risk-taking behaviours. Non-verbal active listening techniques were employed by the interviewer.22
Qualitative Methods
Thematic analysis was chosen for synthesizing key concepts or themes surrounding mental health that were embedded into the narratives provided by parents, students, and teachers in the rural and city location in Bangladesh. Thematic synthesis was rooted in the research tradition of grounded theory and therefore, the themes are grounded in the data itself.23 This method consists of three stages 1) coding text 2) developing descriptive theme headings called ‘categories’ and 3) generating analytical themes referred to as ‘themes’ that can be generically explained.23 Themes were independently drawn from the data grounded in the narrative by all authors on an independent basis. Themes identified were found to be consistent between researchers. In the inductive analysis, emphasis was on categories as opposed to exact words or wording used due to 60.7% of interviews requiring translation from Bangla into English.
Primary translation of the recorded interview had been performed by the field researcher. An anonymised version of each recorded interview was further sent to an independent translator that verified the content of the transcripts. Any discrepancies were removed from the analysis. Translated transcripts were provided to all researchers for thematic analysis and coding purposes.
Written narrative from teachers were not compared against the verbal narrative from parents but narrative was explored within these separate groups. Data collated from students and parents in rural locations where compared against student and parents in city locations, respectively.
Because stressful events are associated with mental health24 and the neurological response to stress is a significant biological factor associated with the onset of mental health disorders,25 narratives were explored for experiences of traumatic or stressful events that may have had a noticeable impact on the student, from the student perspective and from the parent perspective.
RESULTS
Demographics
Demographic data can be viewed in Table 1. Please note, four rural student respondents failed to provide an age and five rural parent respondents indicated that their age was not known or known (as oppose to leaving no response). It was known that all student respondents were aged between 7 and 14-years of age.
| Table 1. Demographic Data Collected from Student and Parent Respondents |
|
Demographic Data
|
Frequency (n) |
Mean±SD
Or Percent
|
|
Students
|
Rural |
City |
Rural |
City
|
| Gender |
| Male |
8
|
3 |
47.1% |
50%
|
| Female |
9
|
3 |
52.9% |
50%
|
| Total |
17
|
6 |
100% |
100%
|
| Age |
| Male |
7
|
3 |
11.00 ±2.09 |
10.67±2.08
|
| Female |
6
|
3 |
10.57±2.51 |
9.67±3.05
|
| Total |
13
|
6 |
10.77±2.24 |
10.16±2.40
|
| Educational Plan |
| Compulsory Education Only |
17
|
6 |
100% |
100%
|
| High School Graduate |
1
|
6 |
5.88% |
100%
|
| Further Education |
1
|
6 |
5.88% |
100%
|
| University |
0
|
6 |
0% |
100%
|
| Post Graduate |
0
|
2 |
0% |
29%
|
| First Language |
| English |
1
|
6 |
6% |
100%
|
| Bangla |
16
|
0 |
94% |
0%
|
|
Parents
|
Rural |
City |
Rural |
City
|
| Gender |
| Male |
7
|
3 |
38.89% |
50%
|
| Female |
11
|
3 |
61.11% |
50%
|
| Total |
18
|
6 |
100% |
100%
|
| Age |
| Male |
5 |
3 |
48.75±13.74 |
45.33±8.33
|
| Female |
8
|
3 |
35±7.94 |
43.00±5.57
|
| Unknown |
5
|
0 |
– |
–
|
| Total |
18
|
6 |
42.85±13.01 |
44.16±6.46
|
| Highest Educational Attainment |
| Unable to read or write |
14
|
– |
77% |
–
|
| No Schooling |
16
|
– |
89% |
–
|
| Compulsory Education Only* |
1
|
– |
5.55% |
–
|
| High School Graduate |
–
|
– |
– |
–
|
| Further Education |
– |
– |
– |
–
|
| University |
–
|
– |
– |
100%
|
| Post Graduate |
–
|
– |
– |
60%
|
| First Language |
|
English
|
– |
5 |
0% |
83.30%
|
| Bangla |
100%
|
1 |
100% |
16.70%
|
Statistical Analysis
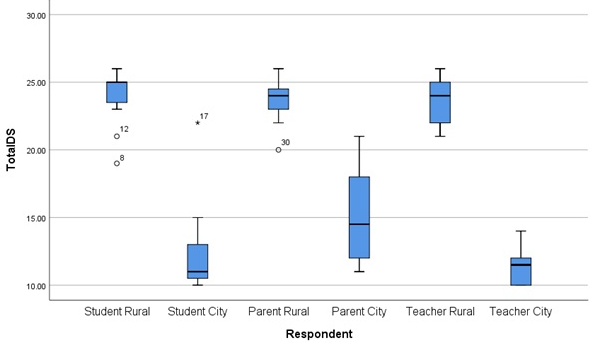
No significant differences in SDQ scores were observed between male and female groups within the rural location or within the city location. Eighty-one percent of respondents reported SDQ total difficulty Scores that were borderline or above. This includes 100% of all scores observed from the rural community and 36.8% observed from the city community.
The difference in observed total difficulty scores between the rural and city school can be seen in the measures of central tendency displayed using a Box Plot (Chart 1). Interestingly, there appears to be a greater variance and distribution of scores within the parent city subgroup. Furthermore, all total difficulty scores observed from the city group appear to be markedly lower than those observed in the rural location.
Chart 1. Box Plot Displaying the Measures of Central Tendency for Total Difficulty Scores (Total DS) for all Respondents in Rural and City Locations
The non-parametric Mann–Whitney U with the Bonferroni correction applied, revealed significant differences were observed in SDQ total difficulties score within the student group between rural and city location schools (U=2.00; Z=-3.67; p=0.000). Significant differences between rural and city student groups were observed in responses hyperactivity (U=13.5; Z=-2.946; p=0.003), conduct problems (U=2.50; Z=-3.80; p=0.000) and emotional symptoms (U=0.000; Z=3.98; p=0.000) subcategory questions, but not with peer problems (U=23.00; Z=-2.28; p=0.027), or prosocial behaviour ((U=35.00; Z=-1.41; p=0.175). Descriptive statistics viewed in Table 2 shows mean±SD, median and variance for the rural and city student subgroups and the associated p values.
| Table 2. Statistical Differences in Total difficulties score Responses Between Student Groups in a Rural Location School and a City Location School (Mean±SD; Median; Variance) |
| Student |
|
Rural (N=16)
|
City (N=7)
|
p
|
|
Mean±SD
|
Median |
Variance |
Mean±SD |
Median |
Variance
|
| Total DS |
24.06±1.84
|
25.00 |
3.396 |
12.86±4.38 |
11.00 |
19.143
|
<0.001
|
| Prosocial |
8.6±1.36
|
9.00 |
1.850 |
7.43±1.90 |
8.00 |
3.619
|
0.175
|
| Hyperactivity |
6.13±0.718
|
6.00 |
0.517 |
3.42±1.82 |
3.00 |
2.619
|
0.003
|
| Peer |
4.88±1.20
|
5.00 |
1.450 |
3.00±1.83 |
2.00 |
3.333
|
0.027
|
| Conduct |
6.5±0.894
|
7.00 |
0.800 |
3.43±0.976 |
3.00 |
0.952
|
<0.001
|
| Emotion |
6.5±0.727
|
7.00 |
0.529 |
3.00±1.00 |
3.00 |
1.000
|
<0.001
|
Significant differences were observed in the total difficulties score within the parent group between rural and city locations (U=1.00; Z=-3.30; p=0.001), and within the teacher group between the rural and city location schools, respectively (U=0.000; Z=-3.57; p=0.001).
The observed SDQ responses from parents in rural and city locations were significantly different in most subcategories of the SDQ scale. Specifically, prosocial behaviour (U=1.00; Z=-3.30; p=0.000), peer problems (U=4.00; Z=-3.40; p=0.001), and emotional symptoms (U=14.00; Z=-3.17; p=0.001) were all observed as showing significant differences. However, there were no significant differences between parent SDQ responses on hyperactivity (U=14.00; Z=-2.27; p=0.041) or conduct problem questions in rural and city communities (U=25.50; Z=-1.03; p=0.304). Descriptive statistics viewed in Table 3 shows mean±SD, median and variance for the rural and city parent subgroups and the associated p values (Table 3).
| Table 3. Statistical Differences in Total difficulties score Responses Between Parent Groups in a Rural and a City Location |
| Parent |
|
Rural (N=12)
|
City (N=6)
|
p
|
|
Mean±SD
|
Median |
Variance |
Mean±SD |
Median
|
Variance
|
| Total DS |
23.58±1.56
|
24.00 |
2.447 |
15.17±3.76 |
14.50
|
14.167
|
<0.001
|
| Prosocial |
9.50±1.00
|
10.00 |
1.000 |
8.00±1.67 |
8.50
|
2.800
|
<0.001
|
| Hyperactivity |
6.42±0.792
|
7.00 |
0.629 |
3.33±1.03 |
3.00
|
1.067
|
0.041
|
| Peer |
5.25±0.965
|
6.00 |
0.932 |
2.67±1.03 |
2.00
|
1.067
|
0.001
|
| Conduct |
5.92±1.24
|
6.00 |
1.538 |
5.17±1.60 |
5.00
|
2.567
|
0.304
|
| Emotion |
6.00±0.853
|
6.00 |
0.727 |
4.00±2.00 |
4.00
|
4.000
|
0.001
|
Teacher responses between the rural school and the city school showed significant differences in all SDQ subcategories, namely prosocial behaviour (U=2.00; Z=-3.45; p=0.000), hyperactivity (U=16.00; Z =-2.50; p=0.016), peer problems (U=2.50: Z=-3.46; p=0.000), conduct problems (U=0.000; Z=-3.46; p=0.000) and emotional symptoms (U=3.00; Z=-3.46; p=0.000). Descriptive statistics viewed in Table 4 shows mean±SD, median and variance for the rural and city teacher subgroups and the associated p values.
| Table 4. Statistical Differences in Total difficulties score Responses Between Teacher Groups in a Rural Location School and a City Location School |
| Teacher |
|
Rural (N=12)
|
City (N=6)
|
p
|
|
Mean±SD
|
Median |
Variance |
Mean±SD |
Median
|
Variance
|
| Total DS |
23.62±1.54
|
24.00 |
2.383 |
11.50±1.52 |
11.50
|
2.300
|
<0.001
|
| Prosocial |
8.00±1.26
|
8.00 |
1.600 |
4.67±0.82 |
4.50
|
0.667
|
<0.001
|
| Hyperactivity |
5.81±0.981
|
6.00 |
0.963 |
4.17±1.33 |
5.00
|
1.767
|
<0.001
|
| Peer |
5.12±0.885
|
5.00 |
0.783 |
1.83±1.12 |
1.50
|
1.367
|
<0.001
|
| Conduct |
6.38±0.806
|
7.00 |
0.650 |
2.50±0.548 |
2.50
|
0.300
|
<0.001
|
| Emotion |
6.31±1.01
|
6.50 |
1.029 |
3.00±0.894 |
3.00
|
0.800
|
<0.001
|
Thematic Analysis
A thematic analysis was performed on the narrative provided by the transcripts observed from the semi-structures interview responses collated from all parents (n=15; rural n=10; city n=5) and all students (n=14; rural n=8; city=6).
Interestingly, all teachers and all city-based respondents chose to speak in English, whereas all rural parents spoke in Bengali as well as 75% of rural students.
Mental Health
The term ‘mental health’ was not understood by 91.6% of parents in the rural location of Bangladesh, Only one rural respondent attributed an incorrect meaning to mental health as ‘immoral development’ in the context of ‘young boys playing card games’. In contrast, 100% city parents viewed mental health as ‘social dysfunction’ with young people being identified as lacking abilities to ‘do’ something, whilst displaying ‘strange’ or ‘immoral’ behaviours that ‘make others feel uncomfortable’. For all teachers and city parents, all underlying aetiology of all mental health disorders were attributed to ‘lack of family bonding’. This is seen as a limited understanding of mental health.
The city teacher’s written narrative showed confusion and conflict in their understanding of mental health. ‘Mental health’ is seen as ‘similar to physical health’ by all teachers, showing an understanding that everyone has mental health, and implying that people can improve their mental health, as they do their physical health. However, all teachers report that any mental health ‘abnormality’ is caused by a ‘lack of bonding’ and, as one teacher reported, this inhibits a child’s ability to ‘cope with other people’. Ninety four percent of rural and 100% of city teachers felt removed from ‘family matters’ and therefore, mental health prevention is seen as largely outside their remit. The observed behaviour of students that are seen to be ‘struggling’ are described using phrases such as ‘different’, behave in a bad way’, ‘act deliberately’ and show a ‘refusal to share’ their thoughts with others. These singular comments collectively show a clear lack of understanding of what mental health means for someone.
Risk Taking Behaviours
There was no report of any risk-taking behaviours by any respondent other than the generic written narrative provided by two teachers. A city teacher noted that students have experienced ‘pressures from teachers, parents or peers’ that have caused ‘negative behaviours’ towards themselves and others. A rural teacher noted changes in ‘violent’ behaviour and ‘also suicide’. Both teachers noted this was related to ‘family bonding’ and the city teacher indicated that this ‘was not a school matter’. This implies that teachers will be unable to support a student in mental health crisis, that may self-harms or has suicidal ideation.
In the city location, 67% teachers factually report policy-type narrative, explaining that the school had two types of support for students, a ‘medical counsellor’ and a ‘moralities counsellor’. This would imply that risk-taking behaviours are required to fall in one of these categories and diminishes the importance of other aspects of mental health.
Learning Difficulties
Classroom strategies are not based on assessments of need and interestingly, no respondent used any of the key terms: dyslexia, dyscalculia, dyspraxia, autism, attention/focus, hyperactivity, cognitive/cognition, auditory or processing.
Learning difficulties was not conceptually understood by the parents in the rural locations. The notion of ‘learning difficulties’ appeared absent from the vocabulary of 100% of rural parents. Any educational or difficulties in learning that their child was having at school was considered a school issue by 100% of rural parents, and 88% of them believed that teachers could ‘fix’ these issues. Eighty one percent of rural students reported that they were ‘badly behaved’ and needed to ‘try better’ when they struggled to learn.
All city parents understood that learning difficulties are associated with using ‘visual aids’ and the responsibility of a student’s learning was joint between parents and school. All city students used the term ‘visual aids’ when being asked about learning difficulties, 83% of city students reported needing ‘visual aids’ to help them learn, and 67% thought they required additional time ‘to make sense’ of their work.
All teachers recognise that some children require additional support and used the term ‘visual aid’. Thirty three percent of city teachers reported ‘unmet needs’ without any further disclosure. One city teacher noted teaching is ‘book and classroom based’ which ‘made students think they are not good’. Eighty three percent of city teachers provided narrative that ‘learning needs’ involved a student being unable to do something, such as ‘they can’t talk properly’, or does something ‘wrong’, such as they display ‘immoral behaviour’. Similar, 67% rural teachers indicate students are ‘unable’ to do something, such as ‘unable to learn equally’.
Attendance
Sixty-seven percent of rural parents reported that their child has regular school attendance, whereas 22% indicated that absenteeism was related to working ‘in the field’ and ‘childcare responsibilities’. One rural parent explained that her son played cricket or football with friends. Consistently, 22% rural students attributed their absenteeism to ‘working in the field’ and ‘childcare responsibilities. One student explained they preferred playing cricket, which was done to occupy his younger sibling whilst the rest of the family ‘worked in the field’.
Eighty-eight percent of rural parents reported more than three offspring and only sent the one child to school. This was always related to ‘hidden costs’, such as uniform and stationary. 38% explained the other siblings helped work in the field as the cost of food for the family was a bigger priority than school.
There was no written narrative on attendance provided by city teachers other than ticking a box, indicating attendance as ‘excellent’. Consistently, city parents explained that their child attended school regularly, 80% of which noted that it was important. All city student respondents said they attended school regularly.
Educational Values
All parents felt education and school was important and agreed that their child was happy in school. The rhetoric used by rural parents was that education was important to ‘get a job in the city’ whereas city parents explained school was important for their child’s development.
There was a direct contrast in parental experiences of education. Eighty-nine percent of rural parents had no formal education, 55% claimed they were unable to read or write but could write their name and 22% claimed they were unable to read or write and unable to write their name. Only one rural parent had received some form of schooling during childhood. In contrast, all city parents had completed a University degree and 60% completed a University Master’s Degree.
All students valued education and saw it as important and were happy at school. Interestingly, all rural students stated that their worst subject was English whereas 100% city students said their worst subject was Bangla. Favourite subjects for 100% rural students was Bangla whereas the city student’s favourite subjects included English (50%), Maths (33%) or (17%) Science. All city students believed they were clever whereas only 50% rural students believed they were clever.
Aspirations
Only parents and students were asked about aspirations. The concept of ‘aspirations’ needed to be explained to 89% rural parents, all of whom believed they would grow up and work in the field. Seventy-right percent of rural parents explain that they never knew about aspiration and believed they had ‘no choice’. All rural parents believed that since they had no formal education, they could only work in the field. Interestingly, all rural parents hoped that their child, who was receiving an education would be ‘good enough’ and ‘work hard enough’ to work in the city. Zero rural parents could explain what specific jobs were available in the city other than ‘office’ work.
The aspirations of rural students appeared to be linked to ‘serving’ the community whereas city students used rhetoric associated with personal enjoyment or financial reward. All rural students had aspirations: Thirty-eight percent ‘hoped’ to work in an office in the city, 38% ‘hoped’ to be a government official, one ‘hoped’ to be a teacher in a rural community and one ‘hoped’ to be a doctor within the rural community as ‘we don’t have doctors here’. All rural students indicated that these aspirations were not spoken about at home. No rural student provided rhetoric about money or finance. All city students had aspirations: One student indicated that they ‘want’ to be a ‘heart surgeon’, one stated that they ‘want’ to be a ‘famous cricketer’, two wanted to run a ‘business’ to ‘make money’, one ‘wants’ to be a fashion designer and one ‘would like to’ work in government and ‘serve others’. All city students explain that these aspirations are regularly spoken about at home.
Problems in the Community
All parents were asked what they believed the main problems were when raising children in their community. Sixty-three percent of rural parents provided a narrative related to poverty; not having enough money to buy food or clothes or to get your child to school. Twenty-five percent of provided the narrative that poverty stops a child attending education because they are required to ‘work in the field’. Fifty percent claimed children ‘do not listen’ and one parent explained the main difficulty with raising children in her community is the ‘immoral’ activity of young boys playing card games.
Sixty percent of city parents are worried about not having enough time with their children. Forty percent of city parents indicated that they had to rely on others to provide childcare, such as maids and family members. Interestingly, 40% of city parents also indicated that ‘maids’ had more time with their child than they do. Only one parent believed that their child ‘did not listen’ and that this was a problem.
DISCUSSION
The relevant findings of this study showed that students identified from the rural and city school in Bangladesh scored high SDQ scores, although these scores were significantly higher in rural location than in the city location. These scores are supported by data collated from the parent and student interviews and suggest a high level of mental health need in both the rural and city location. What is worrying is that, given the high SDQ scores observed, parents in rural locations do not know what mental health is and parents in the city location, as well as all teachers, see mental health only in terms of ‘lack of bonding’. The authors believe this view of mental health is severely limiting. We know from previous studies that lack of understanding or limited understanding on issues related to mental health is associated with the development and maintenance of stigmatization.8,18
The concept that mental health was caused bya ‘lack of bonding’ and ‘family insecurities’ was a consistent findings that could be related to insecure attachment theory, whereby a primary attachment bond is broken or contaminated by fear.26 Whilst this notion provides some insight into the development of mental health issues, these factors alone represent a limited understanding of mental health is and could possibly increase stigmatization, thus inhibiting a young person from seeking help.8,18 For example, using attachment theory alone for all mental health issues implies students with secure attachments will not have any mental health issues. This represents a form of stigmatization that has developed through limited understanding.8 Therefore, to reduce the indirect stigmatization that is likely to be present through lack of or limited understanding, one immediate implication of this study, is the delivery of mental health advocacy within these specific schools as our next step. The authors believe this is an essential and immediate outcome of this specific research.
The authors would like to point out, they are not indicating that mental health conditions are caused by communities having a lack of or limited understanding of mental health issues or conditions, but, in line with previous literature, firmly believe that these factors are associated with increased stigmatization which can prevent young people from talking about their mental health and prevent them seeking help.2–20
This research highlights the attitudes and understanding of mental health as well as learning difficulties from the parent and teacher perspective as well as the student perspective. This study highlights the differences in priorities between parents living in a city community and parents living in a rural community that is socio-economical deprived. Research focusing on stigmatisation and discrimination towards those with mental health disorders, particularly with the co-morbidity of learning difficulties, in LMICs is conspicuous.2-9,11-20 Research has focused on the detrimental impact on individuals with a mental health condition, as opposed to the understanding or conceptualisation of mental health as a construct itself.2-9,11-20 However, by focusing purely of the service user’s perspective of stigma and not those represented by the wider community, including the ‘discriminators’, will fail those with mental health issues that require family and community based support in the absence of mental health professionals. Therefore, our research supports the notion that mental health advocacy and awareness is a primary priority in preventative strategy to support mental health and well-being within LMICs.
Subsidiary findings of this study show that ‘storytelling’ is currently being used within the classroom environment to support the mental health and well-being of students. Therefore, ‘storytelling’ would be accepted as a therapeutic tool. Storytelling has been found to improve cognitive reappraisal27 which promotes emotional regulation and this educational teaching strategy would be particularly useful for anxiety disorders.27 The use of ‘story telling’ was also used by a city teacher, but as a memory aid. Story telling can support the retrieval of long-term memory and improve the speed of working memory.28 Using story telling as a memory tool improves problem solving-abilities which is associated with improved mental health and greater efficiency in the ability to make and change schemas.28 With this is mind, the authors look towards developing a ‘storytelling’ intervention tool to work directly with this cohort group that encourages young people to talk about their emotions and feelings.
No respondent quantifiably attributed any risk-taking behaviour to any specific student. This contradicted written narrative provided by two teachers on generic risk-taking behaviours. One teacher adamantly denied that any of their students would engage in ‘immoral risk-taking behaviour’. This adamant denial lacked consistency with the two other teachers who sign posted the mental health service provision of the school, as well as the report of ‘violence’ and ‘also suicide’. Although not known, the researchers believe this denial may be symptomatic of stigmatization which would prevent students from seeking mental health support, increasing the likelihood of self-harm and suicide. Interestingly, more than 8,00,000 people die from suicide worldwide in every year2 and in Bangladesh, there are 8.7 deaths from suicide for every 1,00,000 females and 6.8 deaths from suicide for every 1,00,000 males.17 The authors believe that this is worth further exploration.
There are known socio-economic factors that divide rural and city communities in Bangledesh.17,29 This notion supports our findings that only rural parents were seen to manage the conflict whether sending their child to school was more important than putting food on the table. Therefore, to support the primary prevention of mental health, we need to understand mental health and well-being in the environment and context in which they exist.30 If mental health is higher amongst students within the rural community, then its key narrative is appears to be poverty. Although we cannot eliminate poverty, we can encourage the development of the relationship between student and teacher, and school and parent; we can provide an understanding of what mental health is and how to support someone who is struggling with their mental health and well-being within their existing communities. Although mental health awareness is necessary to move forward, the findings of this study also suggest action to further support rural communities is essential.
The authors accept that this study has significant limitations. The research data collated was cut short by COVID-19, prompting a variation and a weakening in design. The sample used was small and the parameters for using parametric statistical analysis was not met. Therefore, any generalisations made should be approached with extreme caution. Furthermore, there was a significant language barrier, causing discrepancies between interpretations and the further loss of data. However, what remains fundamental is that this study emphasises a need for further, more robust research where there is a high need and little in the way of mental health resources or understanding.
CONCLUSION
This study found high mental health needs in both a rural and a city school located in Bangladesh. Despite both schools showing a high prevalence of mental health needs, the results showed that overall mental health needs in the rural location was significantly higher than in the city location. These are preliminary findings based on the results observed in the SDQ scores from teachers, parents and students as well as from the parent and student interviews. Written narrative received from teachers were also considered. This study also showed that rural parents within this study lack an understanding about what mental health is and that city parents and all teachers struggle with a limited understanding of what mental health is, attributing the causes of mental health to ‘family bonding’ alone. We do not know if this leads to mental health stigmatization but our findings support other studies that suggest it is likely to. If this is the case, this would prevent a student seeking out mental health help and support within these schools.
ACKNOWLEDGEMENT
The research was funded by Muslim Hands. The authors wish to thank Eleanor Ryan-Haynes for her research contribution.
CONTRIBUTORS
ZT, LEO: Conceived, planned and oversaw the study; designed questionnaires and semi-structured interviews, methodology. KC: field researcher, interpretation from Bengali to English. LEO: Statistical arrangement and analysis, Transcribing, Thematic analysis, writing of the original draft manuscript. ERH: Data inputting, transcribing, thematic validation. VSL: Thematic validation. Disagreement between researchers were resolved by consensus between LEO, ERH and VSL. All authors reviewed, commented on, and approved manuscript.
CONFLICTS OF INTEREST
The authors declare that they have no conflicts of interest.


