INTRODUCTION
Institution based, services are unable to meet the present need of the Indian population because of a large patient load spread across a wide area.1 Health camps, on the other hand, have the advantage and flexibility of delivering healthcare to the patients at their doorsteps, however, the quality of care often becomes an area of concern. This is because the health camps are primarily supervised by junior clinicians, whereas more senior doctors with greater expertise are out of reach for a large percentage of the population.
To address this need telemedicine has a definite role.2-4 Telemedicine is the use of telecommunication and information technology to provide clinical health care from a distance. It has been used to overcome distance barriers and to improve access to medical services. Various modalities have been used in medical education and in recent times provide remotely located people the opportunity to interact with national and international experts in the field of medicine.5,6
The digital stethoscope is a simple instrument that converts sound to a digital signal that is then transmitted and reconverted to a sound signal that can be heard by a more experienced clinician located elsewhere. In this article, we describe the use of the digital stethoscope in a health camp setting.
METHODOLOGY
This study was conducted in health camps organized by the department of plastic surgery of a tertiary care centre in 2019. Outreach Camps covered around 200 kilometers including 5 rural areas. Most of these rural regions were about 150 kilometers from the tertiary centre. A total of 26 patients were screened. Informed written and verbal consent was obtained from the patients.
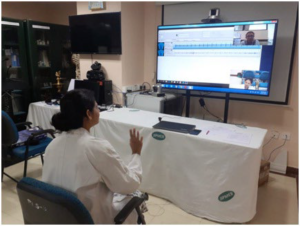
A teleconsultation room consisting of a laptop with builtin speaker/smartphone and internet (Dongle data card) was setup. Likewise, senior consultants were provided a teleconsultation room as well. Using free video calling applications, resident/junior doctors were connected to remote consultants who provided them with guidance and consultation (Figure 1). The junior doctor used a digital stethoscope (3M Littmann Electronic Stethoscope model3200) for auscultation of heart sounds. The 3M™ Littmann® Electronic Stethoscope model 3200 (Figures 2 and 3) picks up sounds, such as heart and lung sounds, from a patient’s body. After amplification and filtering, the sounds are sent to the user through a binaural headset. The stethoscope chest piece is designed for use with adult, pediatric and infant patients.
Figure 1. A Doctor at a Health Camp Using a Digital Stethoscope

Figure 2. A Digital Stethoscope with USB Memory Chip

Figure 3. An Example of the Software Required to Interface the Digital Stethoscope with the Laptop
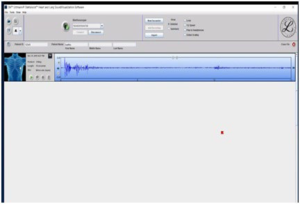
The user interface for the stethoscope includes a 5-button keypad and an liquid crystal display (LCD) display. Sound processing is carried out with the aid of a digital signal processor. Stethoscope power is provided by a single AA battery in the chest piece. A power management system is included to prolong battery life. Using its bluetooth wireless link, the stethoscope can exchange audio data with an external device such as a personal computer (PC) having installed software provided by the company (Figure 4). Data was transmitted over a bluetooth connection to the laptop equipped with the 3M™ Littmann® TeleSteth™ System software (Figures 2 and 3). The laptop screen was shared by video conferencing with a senior physician who provided consultation based on the auscultatory finding (Figure 5).
Figure 4. A Digital Stethoscope with USB Memory Chip

Figure 5. A Senior Doctor Performing a Teleconsultation
Patients and doctors were asked to rate the experience on a scale of 1 to 5 rating, the higher the score the more was the satisfaction level. Feedback statement was also taken from doctors and patients (Table 1). For patient experience was rated based on satisfaction with their consultation, time saved and money saved. For doctors, the experience was rated based on the experience of learning a new tool, quality of sound, ease of using the instrument.
| Table 1. Feedback Form |
|
Questionnaire
|
Rating 1 to 5
(1 being worst, 5 being best)
|
| How was audio quality |
|
| How was video quality |
|
| How was overall quality of live interaction |
|
| How was the experience with this new
device |
|
| Would you like to recommend other for
usage of this device |
Yes/No
|
| Suggestions, if any:- |
RESULTS
Feedback was obtained from patients, and junior doctors at the health camps and from senior consulting doctors located remotely. All the patients (100%) were satisfied with their consultation and agreed that their time and money are saved by attending the telehealth camp. All the junior/resident doctors (100%) felt they had a satisfactory learning experience and all of them were satisfied in the consultations they received. Although no abnormal heart sounds were detected in any patient during these health camps, the junior doctors found the digital stethoscope to be user friendly of educational value. Likewise, the senior consultants also found it very helpful. (Tables 2 and 3).
| Table 2. Patient Satisfaction Score (1 lowest, 5 highest) |
|
Patient
|
Experience rating
|
|
1
|
5
|
|
2
|
4
|
|
3
|
5
|
|
4
|
3
|
|
5
|
3
|
|
6
|
5
|
|
7
|
4
|
|
8
|
4
|
|
9
|
4
|
|
10
|
5
|
|
11
|
3
|
|
12
|
4
|
|
13
|
5
|
|
14
|
3
|
|
15
|
3
|
|
16
|
4
|
|
17
|
5
|
|
18
|
4
|
|
19
|
5
|
|
20
|
5
|
|
21
|
3
|
|
22
|
4
|
|
23
|
5
|
|
24
|
4
|
|
25
|
4
|
|
26
|
4
|
| Table 3. Patient Satisfaction Ratings (1 lowest, 5 highest) |
|
Physician
|
Experience rating
|
| Senior Consultant |
5
|
| Junior doctor-1 |
4
|
| Junior doctor-2 |
5
|
| Junior doctor-3 |
5
|
| Junior doctor-4 |
5
|
| Junior doctor-5 |
5
|
| Junior doctor-6 |
5
|
DISCUSSION
Health care in India is as it stands currently, cannot provide specialist/expert care to the majority of patients in need. Health camps are conducted frequently to overcome this problem. These health camps are often conducted in remote areas with very limited connectivity to main city. Patients typically travel a long distance with limited means of public transportation. Travel costs accumulate due to travel distance and frequently being accompanied by relatives. Telehealth camps provide health care much closer to the patient resulting in a reduction in both travel time and cost. In the case of this study, a reduction in travel time of 2-3-hours, and cost saving of approximately 500-1000 Indian rupee (INR).
As these health camps are often staffed by junior doctors this may lead to under or over diagnosis of certain medical conditions. A telehealth camp, which uses telemedicine, is new idea in which telecommunication and information technology is used to provide specialty health care from a distance.7-10
The digital stethoscope is simple instrument that converts sound to digital signals. The signals are transmitted via the internet remotely over internet and can be interpreted by a physician elsewhere. The advantages of a digital stethoscope include ease of use, amplification of sound, and noise reduction filters. The primary limitation of such a device is the cost (>50,000 INR).
Although this study detected no cardiac auscultatory abnormalities, it did demonstrate the feasibility of such telehealth camps, and greater patient and clinician satisfaction.
CONCLUSION
The digital stethoscope enhances the telehealth camp experience, both for patients and clinicians alike. It saves both time and money for the patient, while providing them with specialty consultations. Larger trials are required to confirm these findings.
DECLARATIONS
Authors’ Contributions
All authors made contributions to the article.
Availability of Data and Materials
Not applicable.
Financial Support and Sponsorship
None.
Consent for Publication
Not applicable.
CONFLICTS OF INTEREST
The authors declare that they have no conflicts of interest.


