INTRODUCTION
The terms overweight and obesity are used for people who weigh more than the recommended limit for their age or gender. Reportedly, these terms are an important risk factor for cardiometabolic diseases, including diabetes, hypertension, dyslipidemia, and coronary heart disease.1 It is also rising to pandemic proportions all over the world.2 Both overweight and obesity have been considered serious health problem throughout many countries since 1997 because the developed and developing countries are continually experiencing increasing rates of overweight and obesity.3 Indication shows that overweight and obesity are the fifth leading risk for global deaths; at least 2-8 million adults pass on each year as a result of being overweight or obese. 44% of the diabetes burden, 23% of the ischemic heart disease, 7% to 41% of certain cancer burdens have been attributable to overweight and obesity.4
Many anthropometric measures have been used in the past to assess overall obesity and central or abdominal obesity, visceral fat, or subcutaneous fat. Computed tomography (CT) and magnetic resonance imaging (MRI) are also applied in the assessment of visceral fat. Dual-energy X-ray absorptiometry is a very reliable alternative approach in the investigation of body adiposity.5 The above approaches for the assessment of excess adiposities (over weight and obesity) are cost intensive,6 and may not be visible in most developing countries where poverty is ravaging their citizens.
Anthropometric measures such as weight and height for calculating body mass index (BMI), waist and hip circumferences (WC and HC) for the calculation of waist/hip ratio are reported to be low-burden standard and effective substitute measures for abdominal adiposity.7
BMI is a frequent screening tool for detecting excess adiposities (obesity/ overweight)8 ; it is calculated as weight in kilo gramme divided by height in meters squared (BMI=weight (kg)/ height (m)2 ).9,10 Obesity and overweight are therefore defined by BMI. This implies weight higher than what is considered normal or healthy for a given height.9,10
Reports have documented that the location of body fat may modify the health implications of BMI because central obesity is generally considered to be a stronger risk factor for cardio-metabolic risk than overall obesity.9 Also, Expert Panel on the Identification, Evaluation, and Treatment of Overweight in Adults, reported that individuals with BMI values between 25 and 29.9 kg/m2 are considered as being overweight while those with values of 30 kg/m2 or higher as obese.12 Despite the ease of the use and the popularity of BMI as an anthropometric screening tool, it is recently becoming increasingly clearer that BMI is not a good proxy for regional adiposity,13 because regional deposition of fat, especially in the upper body segment, is a better predictor of some obesity-related complications, such as hypertension, diabetes, and heart disease.14 Anyanwu and colleagues in their study established thigh circumference (TC) as one of the reliable, simple and cheap tools of determining obesity and cardiovascular disease amongst the Igbos of Nigeria.15
Neck circumference (NC) is a screening measure for overweight and obesity and is observed to have good correlation with age, weight, waist and hip circumferences, waist-to-hip ratio, and BMI for both genders.16 NC has also been proven to be an index for upper-body subcutaneous adipose tissue distribution. It has been evaluated in relation to cardiovascular risk factors in other populations.17
The above report and some other reports associating NC cut off points for assessing overweight and obesity formed the basis for this study.
MATERIALS AND METHODS
Study Area and Sample
The area for the cross-sectional study was in the towns of Nnewi, Onitsha, and Awka in Anambra State, Nigeria. The subjects were drawn from Igbo speaking states of the South-Eastern Nigeria who were resident in Anambra State (see Figures 1, 2, and 3).18,19,20 They comprised of both obese and non-obese adult males and females between the ages of 18 to 45-years, without any history of acquired or genetic adiposity. A total number of 402 individuals (199 males and 203 females) were involved in this study from among long distance drivers, market women, and other individuals with unspecified occupations. Informed consent was taken from all subjects prior to the study. It was confirmed that all subjects were of Igbo origin, meaning that both the parents and grandparents of the subjects were Igbos. All the subjects were examined for enlargement of thyroid gland and, if found positive, were excluded from the study.
Figure 1: Geographical Locations of Igbo Land18
Figure 2: Geographical locations of Anambra State19

Figure 3: Geographical Locations of Local Government Area in Anamba State20
Sample Size Determination
In determining the sample size, a simple random sampling technique was applied which proved to be sufficient to obtain statistically significant correlations between the variables.
Ethical Approval
The ethical approval for this research was obtained from the Ethical Committee, Faculty of Basic Medical Sciences, College of Health Sciences, Nnamdi Azikiwe University, Nnewi Campus, Anambra State, Nigeria.
ANTHROPOMETRICS
The following parameters were determined and recorded.
Height and Weight
Height was obtained using a wall mounted height scale (to the nearest 0.1 cm) with each individual shoeless and head held in Frankfurt horizontal plane. The body weight was obtained using a digital weighing scale (to the nearest 0.1 kg) with each individual shoeless (see Figure 4). BMI was then calculated by dividing weight (kg) with the square of height (m).9,10
Figure 4: Figure Showing How Weight and Height were Measured

Neck Circumference (NC)
This was obtained using an in-elastic 60 inch/150 cm plastic tape produced by Two Roses Limited in Ningbo, China. It was taken in a plane as horizontal as possible, at a point just below the larynx (thyroid cartilage) and perpendicular to the long axis of the neck (the tape line in front of the neck at the same height as the tape line in the back of the neck). While taking this reading the subject was asked to look straight ahead, with shoulders down, but not hunched, see Figure 5. In men with laryngeal prominence (Adam’s apple), the measurement was taken below the prominence.21
Figure 5: Figure Showing How Neck Circumference was Measured

Waist and Hip Circumference (WC and HC)
Waist circumference (cm) was taken horizontally to within 1 mm, using an in-elastic 60 inch/150 cm plastic tape produced by Two Roses Limited in Ningbo, China. The measurement was at midpoint between the costal margin and iliac crest in the mid-axillary line, with the subject standing and at the end of a gentle expiration,22 (see Figure 6). Hip circumference (cm) was measured horizontally, at the level of greater trochanters (standard reference point), with the legs close together,9 see Figure 7. WC was then divided by HC to get the waist-to-hip ratio (WHR). All measurements were taken 2-3 times and average measurement recorded.23,24,25
Figure 6: Figure Showing How Waist Circumference (WC) was Measured

Figure 7: Figure Showing How Hip Circumference (HC) was Measured

STATISTICAL ANALYSIS
The data obtained were recorded in Excel worksheet software and was summarized using descriptive statistics of frequency distribution tables; percentages, mean±standard deviation (SDS), student’s t-test and this was analyzed using computer based software, Statistical Package for Social Sciences (SPSS) version 20.0. Level of significance was considered at p≤0.05.
RESULTS
Table 1 shows the differences between male and female variables. The mean value for the male’s NC is 40.45±2.68 cm while that of the females is 32.71±2.37 cm. Independent sample t-test revealed that there were significant differences in height, BMI, NC, HC and WHR between the genders. Males had a significantly higher mean for height (p<0.05), NC (p<0.05) and WHR (p<0.05) compared to those of the females. However, females had significantly higher BMI (p<0.05) and HC (p<0.05) than the males (see Table 1).
| Table 1. Differences Between Male and Female Variables (N=402) |
|
Parameters
|
Male (n=199) |
Female (n=203) |
t-Value |
p-Value
|
|
Age (years)
|
34.17±8.23 |
32.81±8.08 |
1.663 |
0.097 |
| Weight (kg) |
80.78±15.82 |
79.49±17.52 |
0.773 |
0.440
|
|
Height (m)
|
1.73±0.08 |
1.65±0.07 |
10.752 |
0.000 |
| BMI (kg/m2) |
26.94±4.89 |
29.12±6.30 |
-3.878 |
0.000
|
|
NC (cm)
|
40.45±2.68 |
32.71±2.37 |
30.670 |
0.000 |
| WC (cm) |
93.58±13.83 |
93.04±13.92 |
0.396 |
0.692
|
|
HC (cm)
|
102.92±12.74 |
107.13±13.80 |
-3.182 |
0.002 |
| Waist-Hip Ratio |
0.91±0.08 |
0.87±0.06 |
5.882 |
0.000
|
| BMI=Body mass index, NC=Neck circumference, WC=Waist circumference, HC=Hip circumference, WHR=Waist-Hip Ratio. |
Table 2 represents the BMI classifications of the population. Considering the male subjects, only 1.5% was underweight, 28.1% were overweight while 28.6% were obese. The females had 0.5% as underweight, then 37.4% overweight and 38.4% obese.
| Table 2. BMI Classifications of the Population (n=402) |
|
Obesity
|
Male |
Female
|
|
Frequency
|
Percentage (%) |
Frequency |
Percentage (%)
|
|
Underweight
|
3 |
1.5 |
1 |
0.5 |
| Normal weight |
84 |
42.2 |
48 |
23.6
|
|
Overweight
|
56 |
28.1 |
76 |
37.4 |
| Obese |
56 |
28.1 |
78 |
38.4
|
|
Total
|
199 |
100 |
203 |
100
|
The Pearson correlations (r) between NC with the other anthropometric parameters for the females and males are shown in table 3. Pearson’s correlation showed that neck circumference had a very significant positive correlation with BMI, WC, HC and WHR (p<0.05) for both the males and the females, The correlation between male’s NC (YMNC) and male’s BMI (XMBMI) i.e. r=0.733 was better than that between male’s NC (YMNC) and male’s HC (XMHC) i.e. r=0.532. For the females, the correlation between female’s NC (YFNC) and female’s BMI (XFBMI) i.e. r=0.620 was better than that between female’s NC (YFNC) and female’s HC (XFHC) i.e. r=0.565. The least correlation was seen between NC and WHR in the males and female, r= 0.395 and 0.279 respectively.
| Table 3. Correlation of Neck Circumference with Anthropometric Parameters in the Study Population (n=402) |
|
Correlation
|
Males (n=199) |
Females (n=203)
|
|
Coefficient, r
|
p-Value |
Coefficient, r |
p-Value
|
|
NC vs BMI
|
0.733 |
0.000 |
0.652 |
0.000 |
| NC vs WC |
0.701 |
0.000 |
0.620 |
0.000
|
|
NC vs HC
|
0.532 |
0.000 |
0.565 |
0.000 |
| NC vs WHR |
0.395 |
0.000 |
0.279 |
0.000
|
| BMI=Body mass index, NC=Neck circumference, WC=Waist circumference, HC=Hip circumference, WHR=Waist-Hip Ratio. |
Table 4 shows the grouping of NC, WC and HC according to BMI classification in the males while table 5 shows that of the females. 28.1% of the males were obese according to their NC and WC values (43.23±2.85cm. 107.45±9.00cm respectively). The proportion of females that were obese was 38.4%, (NC=34.44±2.31, WC=105.52±10.76 respectively).
| Table 4. NC, WC and HC Grouped According to BMI Classification in Males |
|
Parameters
|
Males (199)
|
|
Underweight (1.5%)
|
Normal weight (42.2%) |
Overweight (28.1%) |
Obese (28.1%)
|
|
NC
|
40.64±5.54 |
38.84±1.22 |
40.10±1.55 |
43.23±2.85 |
|
WC
|
82.97±9.53 |
83.90±10.27 |
94.81±9.90 |
107.45±9.00 |
| HC |
95.25±6.35 |
96.58±13.75 |
103.89±9.14 |
111.86±8.20
|
| Values in Mean±SD, Standard deviation; UW, Underweight=BMI <18.5; Normal weight=BMI 18.5 to 22.9; OW, Overweight=BMI 23 to 24.9; Obese=BMI>25 NC=Neck circumference, WC=Waist circumference, HC=Hip circumference |
| Table 5. NC, WC and HC Grouped According to BMI Classification in Females |
|
Parameters
|
Females (203)
|
|
Underweight (0.5%)
|
Normal weight (23.6%) |
Overweight (37.4%) |
Obese (38.4%)
|
|
NC
|
29.21 |
30.98±1.35 |
32.08±1.71 |
34.44±2.31 |
|
WC
|
82.55 |
79.39±7.86 |
88.98±8.04 |
105.52±10.76
|
| HC |
99.06 |
94.27±9.02 |
104.22±9.29 |
118.00±11.57
|
| Values in Mean±SD, Standard deviation; UW, Underweight=BMI <18.5; Normal weight=BMI 18.5 to 22.9; OW, Overweight=BMI 23 to 24.9; Obese=BMI>25 NC=Neck circumference, WC=Waist circumference, HC=Hip circumference |
The cut-off point of NC to define overweight and obese subjects for the study population is shown in Table 6. The males had a higher cut-off point than females in both the overweight and obese subjects. The Cut-off point of NC to define obesity in the male subjects was ≥40.50 while that of the female was ≥32.50.
| Table 6. Cut-off Point of NC to Define Overweight and Obese Subjects |
|
Parameters
|
Males (199) |
Females (203)
|
|
Overweight (28.1%)
|
Obese (28.1%) |
Overweight (37.4%) |
Obese (38.4%) |
| NC |
≥39.00 |
≥40.50 |
≥31.00 |
≥32.50
|
| NC=Neck circumference |
The Scatter plot matrix showing the correlations between NC and BMI, NC and WC, NC and HC are shown in figures 8 to 10 respectively for the male and female subjects.
Figure 8: Scatter Plot Showing Correlation Between NC (cm) and BMI (kg/ m2 ) in Male and Female Subjects
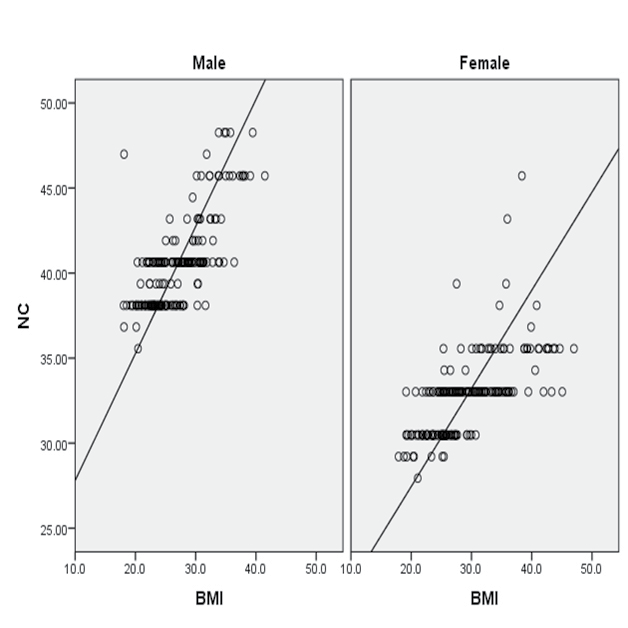
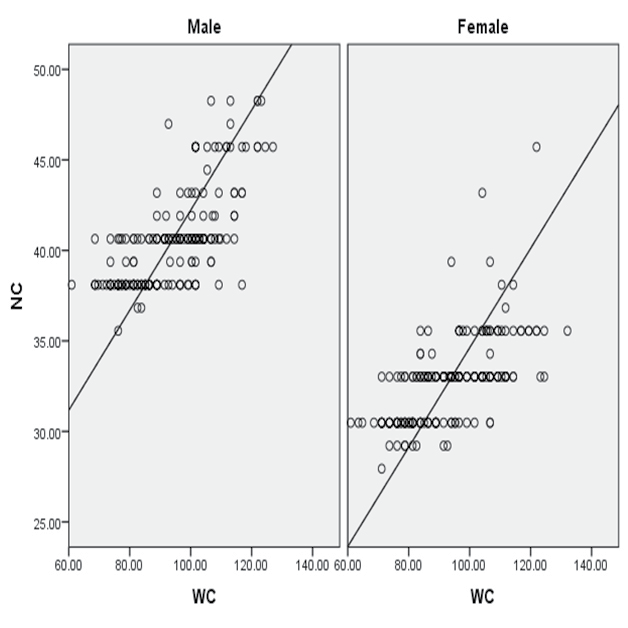
Figure 9: Scatter Plot Showing Correlation Between NC (cm) and WC (cm) in Male and Female Subjects
DISCUSSION
BMI has been identified by most researchers as the most useful epidemiological measure of obesity.3 Studies have shown that the central distribution of body fat cannot be ignored especially in the assessment of body adiposity and obesity; therefore, other anthropometric indices such as thigh circumference (TC),15 waist circumference (WC), hip circumference (HC), waist-hip ratio (WHR)26 have now been used as measures of adiposity. BMI and WC are indices of general and central (visceral) obesity respectively, and are an important first step in determining the level and distribution of obesity,25 however, recent studies have shown that regional (central) adiposity rather than total body fatness is a more serious clinical entity but unfortunately, BMI is a poor descriptor of central adiposity.28
In our study, the anthropometric variables investigated revealed sexual differences and this finding agrees with the report by 23,29,30 that waist circumferences differ in magnitude depending on sex, and are highly reproducible and are correlated with total body and trunk adiposity in a sex dependent manner.
Also in this very study, the mean neck circumference (NC) in males was significantly higher (Table 1) than in females (40.45±2.68 cm vs. 32.71±2.37cm, p<0.000). This is in agreement with previous studies by Adamu and colleagues whose study was based on medical students of Hausa ethnic group (NC= 35.15±1.78 in males and 31.53±2.41 in females),31 Aswathappa and colleagues at RL Jalappa hospital and research centre, Kolar, (NC=36.48±5.70 in males and 34.12±5.70 in females).32 Other anthropometric parameters were significantly higher in males than in females except BMI (26.94±4.89 in males and 29.12±6.30 in females) and HC (102.92±12.74 in males and 107.13±13.80 in females) which is higher in females. This is in agreement with most biological/anthropometric measures where males have significant values than females.33
Pearson’s correlation showed that NC had a very significant positive correlation with BMI, WC, HC and WHR for both the males and the females. The strongest correlation was found between NC and BMI (r=0.733 for males and r=0.652 for females; each p<0.000); this was followed by WC (r=0.701 for males and r=0.620 for females). This is also in agreement with the findings of Ben-Noun and colleagues in southern Israeli (BMI; men, r=0.83; women, r=0.71; each, p<0.0001).16 Our finding is also in concordance with that of Ynag and colleagues on Beijing community and Moazezi and colleagues in patients with diabetes.34,35
The participants, both male and female, were divided into underweight (UW), normal weight (NW), overweight (OW), and obese (O) categories using BMI as the index. Mean NC, WC and HC values in each category were also recorded (Table 5). Male and female subjects in these categories were as follows: Males; UW=1.5%, NW=42.2%, OW=28.1%, O=28.1%. Females; UW=0.5%, NW=23.6%, OW=37.4%, O=38.4%. The overall percentages of male and female subjects that where overweight/obese was found to be 56.2% and 75.8%, respectively.
To evaluate obesity with neck circumference a reliable cutoff point should be determined for men and women discretely.24 In this study, the cutoff points of NC for obesity (BMI≥30) was 40.50 cm for males and 32.50 cm for females (Table 6), which slightly corresponded with the cutoff points (40.75 in men and 35.75 in women) in north Iran.35 Ben-Noun and colleagues in Israel found a cut-off point of 39.5 for men and 36.5 for women.16 In Chinese study, Yang and colleagues also found the best cut-offpoint of neck circumference for central obesity in men to be equal to 37 cm and in women equal to 35 cm.34 Onat and colleagues in Turkey also estimated cut-off points for abdominal obesity (waist circumference ≥95.88) and found that neck circumference of 38.5 cm in men and 34.5 cm in women were the best cut-off points for central obesity.36 Therefore, the NC cutoff points for assessment of overweight and obesity in any given country is gender and population/race specific.
CONCLUSION
Conclusively, this study found that NC had a positive correlation with other anthropometric parameters of obesity especially with BMI and WC, just like other previous studies on correlation of neck circumference with other anthropometric indices. This suggests that NC could be chosen as potential, inexpensive or cost effective and easily measured clinical screening tool for evaluating central (regional) obesity in a local environment with limited budgets on health in other to avert the double burden of adverse adiposities. The results and the cut-off points (both sexes) from this study will be of importance to clinicians and epidemiologists in the diagnosis of obesity and its related adverse effect.
CONFLICTS OF INTEREST
The authors report no conflicts of interest.


