INTRODUCTION
Modern diagnosis made for renal cysts involves knowing how to identify and adequately manage all lesions with the potential of being malignant. Though typical cysts are easily identifiable and are usually benign, it can be difficult to distinguish a complex renal cyst from a cystic renal cell carcinoma or other malignant cystic lesions of the kidney.1 Our work aims to demonstrate that some seemingly benign cysts can actually cover up malignant lesions; hence, it is highly recommended to carefully analyse abdominal computed tomography (CT) scan and to classify each cystic lesion especially when they are multiple.
CASE PRESENTATION
A 78-year-old male moroccan farmer with no significant medical history presented with a 2 year intermittent left flank pain, without macroscopic hematuria nor hydatiduria nor painful urination. Physical examination was unremarkable. Blood analysis especially that of hydatid serology was unremarkable. Abdominal ultrasound showed multiple simple cysts on both kidneys with a suspected left renal cyst that had internal echoes (Figure 1).
Figure 1: Abdominal Ultrasound Showed Multiple Simple Cysts on both Kidneys with a Suspected Left Renal Cyst that had Internal Echoes.

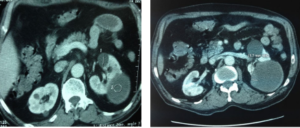
Abdominal CT scan showed multiple cysts on both kidneys with the largest of the cyst on the left kidney estimated to be 7×6 cm with slightly thickened wall classified as Bosniak II F or III, the other existing cysts were all classified as Bosniak 1 (Figures 2 and 3).
Figure 2 and 3: Abdominal CT Scan Showed Multiple Cysts on both Kidneys with the Largest of the Cyst on the Left Kidney Estimated to be 7×6 cm with Slightly Thickened Wall, the other Existing Cysts were all Classified as Bosniak 1.
The patient underwent radical nephrectomy because of the pain and intra-operative conditions, (the major cyst was very close to the vessels). Histopathology of the specimen confirmed papillary carcinoma of the kidney, Fürhman grade 2 cystic alterations, classified as pT2aNx.
Staging found no secondary localizations for this tumor. After a follow-up of 10 months the patient asymptomatic without any sign of recidivism.
DISCUSSION
The vast majority of cystic renal masses are benign. However, malignant tumors may have a cystic appearance. They are dominated by multilocular cystic renal cell carcinomas which are usually low grade.2
Clinical presentation for these lesions is not specific, as in the case of our patient who complained of lower back pain. Diagnosis is often made incidentally during radiological assessment performed for another reason.
Morton Bosniak classification (1986)1 has characteristics that distinguish benign cysts (categories I and II) from potential malignant cysts requiring surgical management (classes III and IV). A new category, called IIF (F for follow-up) was added in 19973 for intermediate lesions between types II and III, requiring regular monitoring through imaging. The relation between Bosniak score and the likelihood of malignancy has been widely demonstrated in the literature.4 However, there is no correlation between the Bosniak score and histological type, TNM staging or Fuhrman grade.4 Although, the lesions found in our patient were classified as type 1 and 2F or 3, nephrectomy was performed due to difficulty in preserving the kidney during surgery. Histopathology study of the specimen revealed the presence of cancer for a renal cyst classified Bosniak II. This implies how important it is to carefully assess the characteristics of multifocal Bosniak I and II cysts.
The Bosniak classification can be adapted to magnetic resonance imaging (MRI) which can at least correlate with histopathological findings.5 Predictive factors of neoplasia are similar to that used in CT scans.1
Contrast enhanced ultrasound of the kidney (CEUS) combines an intravenous injection of gas filled microbubbles to traditional ultrasound, this allows a dynamic study in real time of the enhanced lesion. Several authors describe a higher resolution CT scan with improved sensitivity.6
Renal biopsy in cystic tumors of the kidney is a controversial issue. We did not attempt to perform biopsy in our patient. Indications for renal biopsy remains restricted to Bosniak IV cysts with a tissue target clearly visible on imaging.7 Harisinghani et al7 report that a combination of biopsy and fine needle aspiration of cyst could prevent 40% of unnecessary surgery for Bosniak III cysts. In a series of 199 biopsies associated with a needle puncture for IIF and III lesions, Lang et al1 found a positive predictive value of 91% for malignancy and 100% for benign lesions.1
Typically, non-symptomatic Bosniak I and II do not warrant treatment or special monitoring.
In case of symptoms related to the cyst, treatment can be proposed even for benign lesions2 as this was the case in our patient. Accepted treatment forms are percutaneous puncture and sclerotherapy and surgical resection of the prominent dome.2 We performed nephrectomy as it was technically impossible to preserve the kidney due it’s location.
Bosniak III and IV lesions, as well as evolved Bosniak IIF lesions, should be considered as potentially neoplastic and must undergo surgery by respecting good oncological practice.1,2 The choice between conservative surgery and extended surgery depends on the size of the cyst, its location and the patient’s general condition. Various surgical approaches can be used (open surgery, Coelioscopy or robot-assisted surgery) in our case we performed open surgery because our center is not yet equipped very well with laparoscopy.8,9
CONCLUSION
Benign cystic lesions of the kidney may often not be solely benign as we have reported in our case. This implies a very careful interpretation of available imaging modalities especially that of abdominal CT scans for renal cysts as certain malignant features can be objectified. We recommend surgery without hesitation whenever there is doubt with respect to suspected or doubtful renal cystic lesions.
CONSENT
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editorin-Chief of this journal.
COMPETING INTEREST
The authors declare that they have no competing interests.


