INTRODUCTION
Pelvic actinomycosis is a chronic granulomatous suppurative disease caused by Actinomyces israeli. The opportunistic anaerobic bacterium Actinomycosis israeli is a normal part of the human flora in the oropharynx, gastrointestinal and genital tract.1 More than 50% of actinomycosis infections occur in the craniofacial region. Pelvic infection accounts for 20% of human cases.2 Abdominal-pelvic actinomycosis is often mistaken for other conditions, presenting a pre-operative diagnostic challenge. The infection mimics ovarian tumors and tuberculosis and is diagnosed only after surgery in most of the cases. Actinomycosis secrete proteolytic enzymes, disrupt tissue planes and compress surrounding tissues which makes their presentation closer to a malignant process.3 Slow growing nature of actinomyces, non-specific clinical presentation and extensive spread before the diagnosis is made often pose a clinical challenge. Owing to slow growing nature and chronic inflammatory process, pre-operative diagnosis is difficult and is often made retrospectively after surgical debulking. Infection is rare in infants and children. Many cases are found in women using intra-uterine contraceptive device (IUCD). Actinomycosis is 3 times more common in men than women. Alcoholism, intravenous drug abuse, peptic ulcer, and biliary tract disease are risk factors for actinomycosis.4 It is most commonly found in regions of low socio-economic status and poor hygiene.5 We review a case of pelvic actinomycosis that was managed at the Obstetric and Gynecology Department of K. J. Somaiya Hospital, Mumbai, India.
CASE REPORT
A 50-year-old lady sought gynecological opinion for lower abdominal pain. She gave a history of vague abdominal pain of 6 months which had aggravated over 2 months period. She was post-menopausal since 3 years. Her previous cycles were regular. Our patient was a housewife with 2 children. There was no history of IUCD usage or medical termination of pregnancy (MTP). Patient did not give history of tuberculosis, pelvic inflammatory disease (PID) or any other significant illness in the past. She had history of decreased appetite and loss of 15 kgs of weight over a period of 1 year. On examination patient was pale. Per vaginal examination showed a normal size anteverted uterus with restricted mobility and a vague mass in the left adnexa non-seperable from the uterus. Right fornix was free. No lymphnodes were palpable. Blood investigations showed Hb value of 8.3 gm/dl and ESR-130 mm/1ST hr. Cancer antigen 125 (CA-125) was within normal range. Serial sonographic studies and computerized tomography (CT) scan revealed a irregular high density thick walled heterogenous complex cystic mass lesion in the left adnexa with left ovary not seen seperately from the lesion, measuring 6×6 cms with multiple thin internal echos and small calcifications. Few internal septae dividing the cyst into loculations were also noted. Pre-operatively there was a mass in the left adnexa which was twisted and dense adhesions were seen between adnexa, posterior surface of the uterus and rectum. Mass was separated and intraoperative rupture of mass revealed pus like material. The pre-operative diagnosis was kept of borderline or early malignant ovarian lesion. Total Abdominal Hysterectomy and bilateral salpingo-oophorectomy was done.
The gross specimen showed a left tubo-ovarian mass measuring 7×4×3 cms and cut section showed whitish exudate and granular surface. Endometrium showed a polypoidal thickening throughout. But the uterus, right ovary and tube did not show any significant pathology. Initial histological evaluation revealed dense xanthogranulomatous inflammation with suppurations, eosinophilic abscesses and fungal hyphae with septae and branching, left tube showed lymphoid aggregates and xanthomatous inflammation resembling morphology of fungus aspergillosis. Cytology of ascitic fluid did not detect malignant cells. Patient was initially treated with intravenous ceftriaxone and metronidazole followed by oral therapy for 5 days.
DISCUSSION
Actinomycosis is certainly under-reported as a consequence of diagnostic errors, difficulties in confirming the disease, and the empirical utilization of antibiotics.6 Actinomycosis often presents with vivid presentations that can mimic various etiologies like tuberculosis, nocardiasis, malignancies.6
Our patient was a post-menopausal patient with complex pelvic mass, normal CA-125 levels with raised erythrocyte sedimentation rate (ESR) and history of weight loss, so clinical dilemma between malignant and chronic inflammatory conditions existed. Significant weight loss pointed towards malignant etiology whereas raised ESR suggested of chronic inflammatory condition. Absence of IUCD kept us from diagnosing actinomycosis. Pelvic actinomyces often has complicated presentations as in our case, the mass was pointing towards the malignant etiology. Radiological investigation further added to clinical dilemma with complex tubo-ovarian mass with thick internal echos pointing towards inflammatory condition and loss of tissue planes indicating malignant etiology. Actinomycosis often leads to complex pelvic masses with loss of tissue planes which are difficult to diagnose preoperatively. Intraoperative finding of caseous yellow exudate and pus from the adnexal mass was the 1st objective evidence of inflammatory condition in our case. Failure to diagnose this intraoperatively may lead to extensive debulking surgery as is commonly performed for ovarian cancer with morbidity and loss of organ function. Pelvic actinomycosis has previously been noted to mimic ovarian malignancies. The diagnosis of pelvic actinomycosis is challenging with only 10% of cases diagnosed pre-operatively.2 This is because of a similar presentation to other common conditions such as malignancies, tuberculosis, or Crohn disease.6 Pelvic actinomycosis can occur at any age and in a reported large cohort of 92 patients, the mean age at diagnosis was 37 years.7
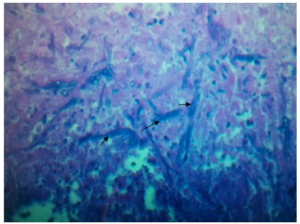
The presenting features usually include fever, pelvic pain or the incidental findings of suspicious pelvic masses on imaging. Ultrasound and CT are the most commonly used imaging modalities for diagnosing pelvic actinomycosis; however, findings are usually nonspecific and thus unreliable in assisting in the differential diagnosis. CT findings in women with abdominal actinomycosis show predominantly solid masses with focal areas of reduced attenuation or thick-walled cystic masses.3 Our patient presented with a unique symptom of vague abdominal pain in combination of significant weight loss. Owing to paucity of clinical clues preoperative diagnosis was in doubt hence with patients of complex tubo-ovarian masses with features unclear of malignant or inflammatory etiology a strong suspicion of actinomycosis should be made. Preoperative diagnosis of actinomycosis in a complex tubo-ovarian mass is difficult owing to difficulty in visualizing actinomyces in routine H&E histopathological sections (Figure 1). actinomyces filaments demand special stains like Grocott-Gomori-Methanamine-silver nitrate stain, Brown-Brenn stain.8 Immunofluroscence techniques also can facilitate actinomyces from tissue sections.9 key point in diagnosing actinomycosis is increases awarness among treating physicians and awareness regarding correct sampling and submission of tissue samples. Actinomyces is susceptible to various anti microbial agents like penicilllin G, erythromycin, clindamycin, chloramphenicol, cephalosporins. Complicated actinomyces infection needs treatment with intravenous penicillin G intensive phase followed by oral penicillin V cover. Patients allergic to penicillin V can be treated with other second line drugs. Owing to chronicity and possible relapse of the condition, long-term antibiotic cover, duration of the same is still not clear.8,9
Figure 1: H&E staining of Tuboovarian mass showing actinomyces filaments.
Combined medico surgical approach helps treating complex actinomyces infection. There are no specific measures to prevent actinomyces, although maintaining personal hygeine, good orodental care, removing dental plaques can help to reduce density if not incidence of colonization.
CONFLICTS OF INTEREST
The authors have declared that they have no conflicts of interest.
CONSENT
The authors have received the written permission for the publication of this case detail.


