INTRODUCTION
Myositis ossificans is a benign condition which appears as a heterotopic, well-defined bone formation in muscles and soft tissues, typically involving muscles, tendons, ligaments, fascia, and aponeurosis.1 It is usually found in children and young athletes. Although the exact etiology remains unclear, it is most commonly reported after major traumatic events, and to larger muscle groups.2 We present a rare case of myositis ossificans in the lumbar spine.
CASE REPORT
A 12 year-old Japanese boy with severe low back pain was hospitalized to our hospital. He was 157 cm tall and 45 kg weight and had no history of sports activities. This low back pain had been restricting his motion more than one month. He had a history of trauma three months ago: he used one of Chinese martial arts at school and practiced nunchak (one of tools of Chinese martial arts). He hit the nunchak on his back. After that, his lower back gradually swollen up and the lower back pain developed afterwards in 2 months. On physical examination, a severe tenderness and swelling was present in the left lumbar region, at levelof L4/5. There was no erythema. The laboratory findings were normal. Neurological examination revealed no motor or sensory deficits, with normal reflexes. Both lumbar radiographs and lumbar Computed Tomography (CT) showed a ring like calcification adjacent to left facet joint of L4/5 (Figures 1 and 2). There was no evidence of bone fracture in the lumbar spine. Lumbar Magnetic Resonance Imaging (MRI) showed high signal intensity area along the left multifidus muscle on T2-weighted axial image (Figure 3A). Short TI Inversion Recovery (STIR) sagittal image showed bone marrow edema at left lamina of L4/5 was demonstrated (Figure 3B). Faint low signal component suggestive of calcification was visualized around the left face joint of L4/5 (Figures 4A and 4B). There was no nerve root signal abnormality. Both clinical and radiological findings were compatible with myositis ossificans. He received conservative treatment. His back pain and swelling disappeared in 2 months. Follow up lumbar CT 8 months later showed calcification became dense as compared to the one in the previous CT (Figure 4). Soft tissue swelling along the left multifidus muscle was improved.
Figure 1: Lumbar radiograph of the patient.
Oblique view of lumbar radiograph shows a ring like calcification at level of L4/5 facet joint (arrow).

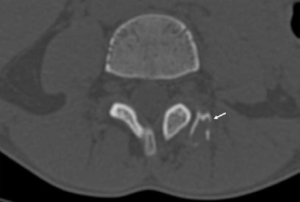
Figure 2: Lumbar CT of the patient.
a. MPR sagittal image shows faint calcification around facet joint at level of L5 (arrow).
b. Axial image shows a ring shape calcification. The left multifidus muscle is swollen.
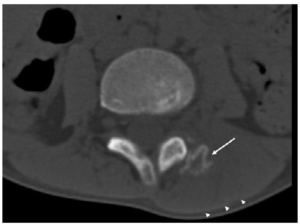
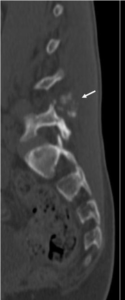
Figure 3: Lumbar MRI of the patient.
a. T2-weighted sagittal image shows high signal intensity area along the left multifidus muscle (arrowheads). Faint low signal intensity structure consisted with calcification is demonstrated around left facet joint of L4-5 (arrow).
b. STIR sagittal image shows focal bone marrow edema in the left lamina of L5 (white arrow). The calcific area forms a low signal intensity ring (black arrow). Left multifidus muscle shows high signal intensity suggestive of inflammatory change.
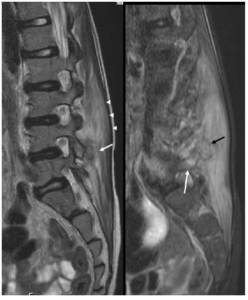
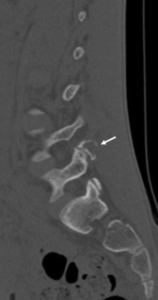
Figure 4: Lumbar CT 8 months later
a. MPR sagittal image. The calcification is more clearly demonstrated as compared to the initial CT examination (arrow).
b. Axial image shows more mature calcification at left vertebral arch (arrow).
DISCUSSION
Most myositis ossificans occur in the large muscles of proximal extremities such as the quadriceps and brachialis. It is rare to occur in the lumber spine. As long as I surveyed, only 3 cases of myositis ossificans in lumbar spine were found on PubMed line.2,3,4 Interestingly, all of the 3 cases had no traumatic history like our case. It could be because the muscle contusion by playing sports might be rarer in the spine than in the extremities. In a small number of cases, possible etiologies include infections, burns, neuro-muscular disorders, hemophilia (factorIX deficiency), tetanus, and drug abuse.5 We should also onsider myositis ossificans if we find these etiologies.
Jocobsen S6 reported from his animal experiments that connective tissue injury of muscle gives stimulation to both fibroblasts and osteoblasts and these cells deposit and structure osteoid centripetally in the lesion. As the lesion matures, cancellous bone develops into mature, lamellar bone in the periphery of the lesion.3 In addition, repetitive minor mechanical injuries, ischemia or inflammation have been implicated as possible causative factors.
In our case, calcification became denser in the followup CT, which is suggestive of mature bone. This change is typical for myositis offificans.
Myositis ossificans is a benign, self-limiting disease. Treatment in most cases is conservative; rest, ice, and antiinflammatory drugs to relieve pain. Typically, a regression of the symptoms is seen in the course of disease (30%).7 Surgical intervention is recommended when the heterotopic bone has matured like our case. The optimum time for a surgery excision is between 9 and 12 month after the trauma.8
CONCLUSION
This case is the rare localization for a myositis ossificans. It was typical findings on CT examination that heterotopic bone had matured.
CONFLICTS OF INTEREST
The authors declare that they have no conflicts of interest.
CONSENT
The patient parents has provided written permission for publication of the case details.


