INTRODUCTION
Chronic cervical pain is a major public health problem that affects approximately 18% of the world population.1,2,3 Treatment guidelines claim that manual therapy techniques such as spinal manipulation are essential for rehabilitation.4,5 The manipulation of cervical spine is highly recommended in cases of cervical pain and stiffness, tension headache and migraine. The technical purpose aims to increase the range of motion, consequently relieve pain by the vertebral repositioning.6,7 Besides being effective in cervical pain complaints, vertebral repositioning is are also indicated in cases of radiculopathy.1,8,9,10,11,12,13
One of the manual therapy technique which promotes the mobilization of nerve roots and acts to test and treat the peripheral nervous system, is the neurodynamic mobilization.14,15 The neural tissue has been pointed as a source radicular symptoms.16 The provocative tests of this tissue are used to identify whether the neural tissue is the cause of pain or not.16,17 These tests consist of a series of passive movements in the affected limb, in order to assess tissue neural mechanics.18 The test is considered to be positive when the symptoms are reproduced during application.19 According to some researchers, the neurodynamic mobilizations do not promote additional benefits when compared with other interventions.20,21 A systematic review shows limited evidence for the use of neurodynamic mobilizations in the treatment of radicular conditions involving the upperlimbs.22 The effects of neurodynamic mobilizations on physiological mechanisms are still unknown in literature and more research regarding these effects may account for its therapeutic effectiveness.23 Even though the association of techniques for treatment of spine disorders is backed by evidence, there are no studies relating the use of manipulation and neurodynamic mobilization in subjects with chronic neck pain.24,25,26 It is believed that spinal manipulation can influence greatly on the answer of the peripheral nervous system tests, thus the objective of this study is to evaluate the influence of spinal manipulation on the Peripheral Nervous System Tests (PNST).27,28
METHODS
Study Design
This study is a randomized controlled trial with blinded evaluator. Consent procedures were approved by the Ethics and Research Committee of the Irmandade da Santa Casa de Misericordia de Sao Paulo, Brazil (Protocol No. 159/10).
Sample Calculation
The sample size calculation for this study was based on a difference of 2 points in the end pain and a difference of 5° on the measurement of the amplitude of movement through goniometry. Using the statistical power of 80%, 5% alpha, and with possible sample loss of 10%, we reached the total of 32 individuals per group, amounting 128 participants.
Participants
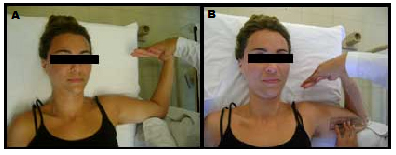
The patient population was composed of males and females aged between 18 to 40 years old, with cervical pain over 12 weeks and positive response (Figures 1 and 2) to peripheral nervous system testing (PNST). Subjects who submitted positive response to the Dekleyn test, underwent spinal manipulation on the previous week, with pain and stiffness in the cervical spine or upper limbs, tension headache, migraine, obese, hypertensive patients, with cervical and/or thoracic osteoarthritis or osteoporosis, chest pain, prior accident in the head or neck, neurologic deficit, Radiculopathy and severe diseases of spine (tumor, fracture and infections), were excluded from the stud.
Figure 1. TPNS for median nerve

A. Initial position of the test. B. Final Position of the test, with goniometry measurement.
Figure 2. TPNS for ulnar nerve
A. Initial position of the test. B. Final Position of the test, with goniometry measurement
The Dekleyn test was performed with the patient supine, with the spine off the stretcher, hyperextended and rotate, for about 1 minute on each side (left and right)17 (Figure 3). This test aims to evaluate the integrity of the basilar artery and insure that it is secure to perform cervical spinal manipulation. The test is considered to be positive when there is the presence of vertigo, nystagmus, dizziness, tinnitus, visual changes, nausea or fainting, indicating insufficiency of the basilar artery, ending the cervical spinal manipulation.17
Figure 3. Dekleyn test

A. Initial position of the Dekleyn test. B. Extension more right inclination C. Extension more right inclination.
The characteristics of the sample (age, gender, weight, high, simptons duration, dominant member, medicantion use, physical activity practice, smoker and visual analogic scale) was collected in baseline.
Evaluation of Peripheral Nervous System Tests
The evaluation of the individuals previously randomized, was performed by blinded evaluator. The evaluator made the PNST to check the involvement of nerve roots of the median nerve and ulnar in positive cases was measured to range of motion by means of a goniometer, where the patient was supine, with the member tested in 90° shoulder abduction and 90° of flexion of elbow, with the fulcrum of the goniometer positioned at the medial epicondyle of the volunteers.17 During the PNST for the median nerve, the volunteer was initially held supine with the shoulder to be tested with abduction of 90° and rotated sideways, with elbow 90° flexion, forearm supinated, wrist and fingers held in extension.17 Below elbow extension was held until the maximum amplitude allowed by the patient and measured the range of motion (Figure 1).17 In PNST for the ulnar nerve, the volunteer was kept in the same position of the median nerve, but with forearm pronated. Below elbow flexion was carried out to the maximum extent permitted by the patient and measured the range of motion (Figure 2).17 Prior to randomization of patients and collecting data, we conducted a pilot study with 10 volunteers (5 men and 5 women), in order to test the reliability of the evaluators about the positioning of the goniometer and handling proposed in the study. The procedures were reassessed after a week. The evaluators presented an intraclass correlation coefficient of 0.87 for the positioning of the goniometer and 0.88 for handling.
Randomization
Patients were randomized into four groups through browns envelopes done by a second evaluator who was the only person aware of which group the patient was allocated and the handling proposal. Blinded evaluator and patients were unaware of the group allocation.
Group A underwent the sixth cervical vertebra manipulation (C6). The patient is positioned supine, with head slightly off the gurney and the therapist conducted a rotation with hyperextension of the segment to be manipulated, by performing a move posterior-anterior (Figure 4). Group B underwent manipulation of the sixth thoracic vertebra (T6). The patient was placed in ventral decubitus, with upper limbs abductees and relaxed for body-worn operation, the therapist positioned both hands parallel to the inferior angle of the scapula region performing cranio-rotational flow pressure (“screw movement”) for implementation of proposal handling (Figure 5). Group C held the combination of groups A and B, manipulation of the vertebras C6 and T6, as described earlier. Group D received placebo manipulation, the patient was positioned in ventral decubitus, upper limbs abductees and relaxed by their sides, the therapist positioned both hands parallel to the inferior angle of the scapula and has not achieved any pressure (Figure 6). After manipulation, patients were reassessed as regards PNST (ulnar nerve and median nerve) goniometry by the blinded assessor. The data collected were sent to statistical analysis.
Figure 4. Neck manipulation

A. Initial position of the neck manipulation. B. Position of the right trust. C. Position of the left trust.
Figure 5. Toracic trust
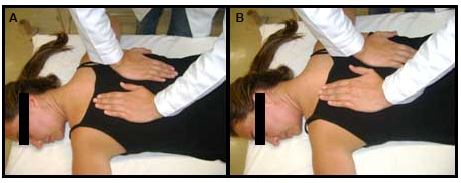
A. Position initial. B. Position final.
Figure 6. Sham trust

The patient position.
Statistical Analysis
For statistical analysis, SPSS 19 and Excel Office 2010 were used. The level of reliability was established at p<0.05. The Wilcoxon test was used to compare the results between periods in each group for the variables measured. The analysis collected by a blinded assessor.
RESULTS
Between the period of April 2011 and December 2012, 182 patient residents in the city of São Paulo were evaluated by the rehabilitation of the Irmandade da Santa Casa de Misericordia de São Paulo. Among the volunteers evaluated, 54 did not comply any of the inclusion criteria and were excluded from the study. An exclusion criterion was: neural test negative (n=19), positive Dekleyn test (n=13) tendinopathy of the supraspinatus muscle (n=8), tendinopathy of the wrist flexors (n=7), previous surgeries in the column (n=6), neurofibromatosis (n=1). The characteristics of patients who participated in the study. Overall this study consisted mostly of women, age of 32 years, weighing 74.5 kg and with an average duration of 15 months of neck pain. As for the dominant side, 82.7% of the population was right-handed and 17.3% were left-handed. There was a significant difference (p=0:03) for the dominant side.
After interventions were complete, the intra-group comparison analysis for the median nerve and ulnar nerve right and left. When analyzed the right median nerve, Group A (p=0.043), handling C6; and Group C (p=0.028); manipulation of the C6 vertebra associated with the manipulation of T6, showed to be significant for the gain of movement amplitude. In the analysis of the left median nerve, as well as the right, the Group A (p=0.03) and Group C (p=0.01), showed significant values for the gain of range of motion. Regarding the variable for PNST right and left ulnar nerve in intra-group comparison, there was a statistically significant difference only in Group A, handling C6, on both sides, right (p=0.04) and left (p=0.03).
DISCUSSION
The objective of this study was to analyze the effects of the manipulation on the peripheral nervous system through PNST of median nerve and ulnar nerve in order to investigate a possible improvement on the range of motion. The choice of C6 and T6 segment for the realization of the manipulation was made according to a study conducted by Butler,17 where they assume the points of reduced vertebral mobility during the flexion movement are the segments of C6, T6 and L4. As the objective of this study was to evaluate the influence of the manipulation in the tests of the peripheral nervous system of the upper limb, only the segment of C6 and T6 were chosen to be tested.
As long as these segments have reduced mobility, end up being more susceptible to form points of tension and develop patologias.13 This rationale confirms the exposed in the study of Christensen and Buswel,13 where it was reported that the cervical Radiculopathy is most prevalent in the seventh nerve root of cervical spine, between C6 and C7 (60%) and in the sixth nerve root of cervical spine, between C5 and C6 (25%). In the variables measured for both the median nerve and ulnar nerve, the groups (C6-handling) and C (C6-handling and T6) feature significant results when compared with the other groups. This may be explained by the fact that 81.2% of the population of the study consisted of right-handed volunteers; but also the methodology established for the study was to initiate the assessment through the peripheral nervous system testing by Member of the volunteer, causing the nerve introduce greater tour tested in neural tube defects when it was tested on the left Member.
But the choice of a control group had aimed to minimize this bias and evaluate if the results achieved were due the manipulations performed or just the fact of having stretched the nerves during the assessment and reassessment of peripheral nervous system tests. As a result, it is possible observe that the control group did not show any improvement in the reassessment of the peripheral nervous system tests. It suggests that handling the C6 vertebra in association with the manipulation of the T6 vertebra, presents better results when compared with the placebo or with only the manipulation of T6 vertebra, since these vertebral regions are considered to have reduced levels of mobility, which can limit the movement of the nerve in the neural tube.
CONCLUSION
Manipulation of the C6 vertebra isolated or associated with manipulation of the T6 vertebra appears to be an effective resource for increasing the range of motion of the median nerve and ulnar nerve. More studies with similar objectives should be carried out, to verify the effectiveness of spinal manipulation on nerve tests of the peripheral nervous system.
CONFLICTS OF INTEREST
The authors declare that they have no conflicts of interest.


