CASE REPORT
A 62-year-old patient presented with gross total painless hematuria and was diagnosed with muscle invasive transitional cell carcinoma of urinary bladder (T2N0M0).
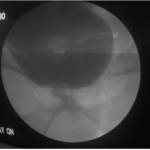
We planned to perform a radical cystoprostatectomy with formation of an orthotopic neobladder. After completing cystoprostatectomy and bilateral lymph node dissection, when we picked and chose terminal ileum for formation of neobladder, incidentally a Meckel’s diverticulum of size 6 cm was found (Figure 1) approximately 28 centimetres from the ileocaecal valve, so we decided to complete detublarisation of selected segment of bowel except Meckel’s diverticulum and to use it for lengthening the neobladder (Figures 2 and 3). Meckels diverticulum was kept at pouch’s most dependent location. After forming a good capacious, near sphere shaped pouch, meckel-urethral anastmosis was done. No major post-operative complications occurred. After removal of the transurethral catheter, the patient voided with good flow. Before removing suprapubic cystostomy tube, cystogram was done which showed bladder, bladder neck and urethra similar in appearance to the native one (Figure 4). At 12-months of followup the neobladder functioned well without residual volume in the neobladder with occasional nocturnal incontinence.
Figure 1. Per-operative Photograph of Ileal Segment with Incidentally Found Meckel’s Diverticulum

Figure 2. Configured Ileal Neobladder with Meckel’s Diverticulum as Neourethra

Figure 3. Bilateral Ureters Reimplanted into the Neobladder with D J Stenting
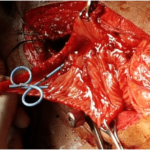
Figure 4. Post-operative Cystourethrogram Mimicking Near Normal Native Bladder And Urethra
DISCUSSION
In review of literature, we found a single case report of using a Meckel’s diverticulum for creation of neobladder in which they found short mesoileum.1 In another case report Meckel’s diverticulum was used for implanting the ureters.2 It has also been used for ureteric repair and as an alternative conduit for the Mitrofanoff procedure.3,4
Meckel’s diverticulum is the most common congenital malformation of the gastrointestinal tract.5 It is an embryologic rest of the omphalomesenteric duct, which normally obliterates in the seventh week of gestation.6 However, it is formed when the intestinal end of the duct remains. Meckel’s diverticulum is normally diagnosed due to a complication, such as a gastrointestinal bleeding in 25 to 50% of the cases or an infection in about 20% of the cases.5 Obstruction, diverticulitis and intussusception are also commonly seen. Symptoms may be due to inflammation and ulceration in a Meckel’s with ectopic gastric or pancreatic tissue.6 However, older patients are unlikely to have such findings.5
Ileal orthotopic neobladder is considered to be the first choice for a continent urinary diversion after radical cystectomy because ileum can easily be manipulated into the pelvis without tension and we can create a low-pressure reservoir which is capacious and continent.7 Using 40 cm of bowel does not result in any malabsorption or any major bowel dysfunction.8,9
The Meckel’s diverticulum we found incidentally was in a very suitable location, and the tip could be easily mobilized into the pelvis. By using the Meckel’s diverticulum we could easily perform an anastomosis with the urethral stump without undue tension. A sphere-shaped pouch was created above the diverticulum. The ureters were implanted laterally into the pouch. This operative technique enabled us to create a good capacious pouch and to reach the urethra without traction. In our opinion, we can safely use the diverticulum if found in the absence of any inflammatory bowel disease.4 To our knowledge, this is the first report on the elective use of a Meckel’s diverticulum in the formation of an orthotopic neobladder.
CONCLUSION
We described the elective use of a Meckel’s diverticulum to lengthen the distal part of an orthotopic neobladder which can be used to create a tension free and relatively easy urethal anastmosis if found incidentally. It may be very useful in case of short mesoileum.
CONSENT
The authors have received written informed consent from the patient.
CONFLICTS OF INTEREST
The authors declare that they have no conflicts of interest.


