INTRODUCTION
The iliopsoas tendon acts a thigh flexor and aids in lateral rotation of the hip. The Iliopsoas injuries are generally considered uncommon. Especially, in children and adolescents, the Iliopsoas injury usually occurs in conjunction with avulsion of the lesser trochanter.1 We report a rare case of a partial tear of the left psoas major tendon in an adolescent patient. The authors obtain written informed consent from the patient for submission of this manuscript for publication.
CASE REPORT
A 14-year-old-male who had a left inguinal pain came to our hospital for consultation. The injury occurred when he was earlier playing a basketball game and turned on a pivot, he suddenly felt left inguinal pain. He is 170 cm tall; 50 kg in weight and has no history of trauma or disease. He has been playing basketball for 5 years at school and plays it for 4 hours every day. On physical examination, there was severe tenderness present in the left inguinal region. Also, there was no erythema. He could not move his left hip joint by himself. Neurological examination revealed no motor or sensory deficits with normal reflexes. The laboratory findings were normal. Hip radiograph showed no abnormality (Figure 1). On MRI, the left psoas major tendon showed up as swollen and was separated from the left iliacus tendon on STIR axial image when compared to the right side (Figure 2). It shows high signal intensity in that area suggestive of hematoma, this is shown between the psoas major muscle and iliacus muscle (Figures 2 and 3). The left psoas major tendon and myotendinous junction showed high signal intensity on STIR coromal image (Figures 3 and 4). In addition, a partial tear of the left psoas major tendon was visualized (Figures 3 and 4). However, the left lesser trochanter and insertion of the left iliopsoas tendon was maintained (Figure 5). The lesser trochanter showed slightly high signal intensity as compared to the opposite side but showed no evidence of avulsion fracture on STIR axial image (Figure 5).
Figure 1. Anterio-posterior View of Hip Radiograph

There is no evidence of bone fracture in the left lesser trochanter (arrows).
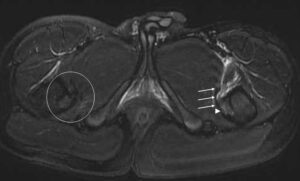
Figure 2. STIR axal hips MRI at Level of Acetabulums

As compared to the right iliopsoas tendon (white circle), the left psoas major tendon (white arrow) showed
swollen and was separated from the left iliacus tendon (black arrow). High signal intensity area
suggestive of hematoma is visualized mainly around the left psoas major muscle.
Figure 3. STIR coronal hips MRI at level of pubic symphysis
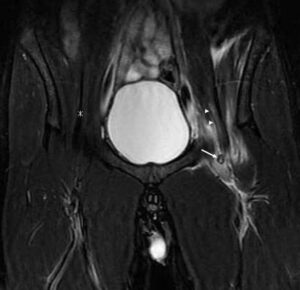
Both the left psoas major tendon (white arrow) and myotendinous junction (arrowheads) show
partial high signal intensity suggestive of tear. The right psoas major tendon (asterisk) is normal.
Figure 4. STIR coronal hips MRI at level of pubic symphysis at level of the 4 mm behind from Figure 3
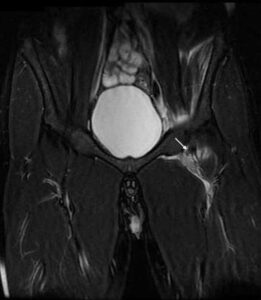
The partial tear of the left psoas major tendon is visualized (white arrow).
High signal intensity hematoma is along the left psoas major tendon.
Figure 5. STIR axial hips MRI at level of both lesser trochanters
Both the left lesser trochanter (arrowhead) shows faint high signal intensity but shows no avulsion fracture.
The insertion of the iliopsoas tendon (arrow) is the same signal and form as the right side (white circle).
We diagnosed a partial tear of the left psoas major myotendinous junction and tendon due to overuse. He was hospitalized and underwent a conservative therapy. He was discharged after a week with no inguinal pain.
DISCUSSION
The Iliopsoas muscle belongs to the inner hip and comprises of a complex of two muscles called psoas major muscle and iliacus muscle. Both muscles pass below the inguinal ligament through the muscular lacuna together and merge at their midpoint to form a common insertion at the lesser trochanter of the femur.1,2,3 The iliopsoas muscle controls the various actions of postural changes such as walking, running, sitting, or standing. It also keeps the upper body straight while one is performing certain types of exercises in the supine position.1,2,4 The Iliopsoas tendon injuries without lesser trochanteric avulsion in children and adolescents are distinctly uncommon, with an estimated prevalence of 0.66%.1,2 An even smaller percentage of these injuries occur spontaneously. This is due to the relative weakness of the apophyses compared to the iliopsoas tendon.5,6 Regarding the epiphyseal union of the lesser tronchanter, Shama Y et al7 reported that age of epiphyseal union of the lesser trochanter was 18-19 in male and women together. Cardoso8 reported that the lesser trochanter at age of 14 of male showed nonunion. In our case, the left lesser trochanter was not fractured but showed faint bone marrow edema. We think the bone marrow edema of the left lesser trochanter occurred as a result of an overload from the left iliopsoas tendon. In addition, we found a partial tear of the left psoas major tendon on MRI. It may be due to the overuse from the patient’s sports activity. In adults, isolated fractures of the lesser trochanter are rare but can occur as a result of trauma or sports injuries like jumping, kicking and so on.3,4 When iliopsoas muscle and tendon are subjected to a load beyond the strength of the muscle, it occurs. The vast majority of ruptures are partial muscle/tendon tears.5,6 Our case is the same as the adults’ iliopsoas muscle injuries. Taking a MRI is a good choice to evaluate iliopsoas tendon injuries and distinguishes it from other hip joints diseases. In our case, we could rule out the lesser trochanteric avulsion on MRI. The iliopsoas muscle/tendon injuries are usually treated conservatively, with rest, physical therapy, and/or antiinflammatory medications, often with good results.1,2
CONCLUSION
Ilippsoas tendon injuries without lesser trochanter avulsion are uncommon in children and adolescents. We need to evaluate both the lessor trochanter and the insertion of the iliopsoas tendon to rule out lesser trochanter avulsion on MRI. The hips MRI is a good modality for distinguish from them.
CONFLICTS OF INTEREST
None.
CONSENT
The authors obtained written informed consent from the patient for submission of this manuscript for publication.


