INTRODUCTION
The normal adult thyroid gland is composed of two lobes joined by the isthmus, which lies across the trachea anteriorly, below the level of the cricoid cartilage.1 The gland is affected in many physiologic and pathologic conditions. Diseases of the thyroid include conditions associated with excessive release of thyroid hormones (hyperthyroidism), thyroid hormone deficiency (hypothyroidism), and mass lesions of the thyroid.2
Thyroid nodules are one of the commonest clinical findings with a reported prevalence of 4-7% in the adult population. Overall, however, only fewer than 5% of adult thyroid nodules are malignant with the vast majority being non-neoplastic lesions or benign neoplasms.3 Selecting those neoplastic nodules among the different lesions is of paramount importance when deciding to operate on the enlarged thyroid.
One of the well-established and preferred first line diagnostic tools in the evaluation of diffuse thyroid lesions as well as of thyroid nodules is fine needle aspiration cytology (FNAC) with the main purpose of confirming benign lesions and thereby, reducing unnecessary surgery.4 FNAC is a safe, inexpensive and accurate diagnostic tool with a sensitivity and specificity, 94% and 98% respectively, with few false positive rates of 3.3%.5
Despite several studies showing a high accuracy of FNAC, studies especially in Eastern Africa and other developing countries with a high prevalence of nodular thyroid disease, have shown the accuracy of FNAC to be lower and its diagnostic performance has been shown to vary across different studies.6 Although the magnitude and prevalence of thyroid disorders were reported in various literatures, histopathologic data and specially diagnostic performance of FNAC in Jimma University Medical Centre (JUMC) is not known. Hence, the purpose of this study is to determine the overall histopathologic patterns and cytohistologic correlation of thyroid lesions using histopathologic examination as the gold standard.
MATERIALS AND METHODS
It is a retrospective study in which, among a total of 8,412 biopsies received from September 2015 to September 2020, conveniently, 582 histopathology reports of thyroidectomy specimens were retrieved from the pathology department data archive and those reports that fulfilled the inclusion criteria were manually selected and then grouped by year. One biopsy report was excluded using exclusion criteria. A total of 286 FNAC results were also obtained from those reports in which FNAC was done prior to surgery. Fine needle aspirations were done for evaluation of palpable thyroid lesions and no image-guided techniques were employed.
Inclusion Criteria
All biopsy reports of patients with the diagnosis of thyroid diseases which are done from September 2015 to September 2020.
Exclusion Criteria
Biopsy reports which do not have all of those variables: patient age, sex, and histologic diagnosis.
Data Collection Procedures
Histopathology reports of biopsies submitted from thyroid lesions to Jimma Medical Centre (JMC), pathology department from September 2015 to September 2020 were retrieved from pathology department data archive. A structured checklist was adopted through reviewing of literature and books to include information that fulfils the objective of the study. Eligible 581 reports fulfilling inclusion and exclusion criteria were extracted and recorded into a prepared checklist containing study variables. A total of 286 FNAC results were obtained using the hard copies (biopsy request papers) and soft copy archive.
Data Analysis
Data analysis was performed using the statistical package for social sciences (SPSS) version 26. Descriptive analysis was done for frequency and distribution of the disease. Cross tabulation, chi square (χ2) test and logistic regression were done to determine the association between the variables. Those variables with a p-value<0.25 in binary logistic regression were recruited for multiple logistic regressions. Then, p-value<0.05 was used as a cut-off point for identifying predictors for histopathologic patterns. The probability value p≤0.05 is considered statistically significant.
RESULTS
Demographic Characteristics
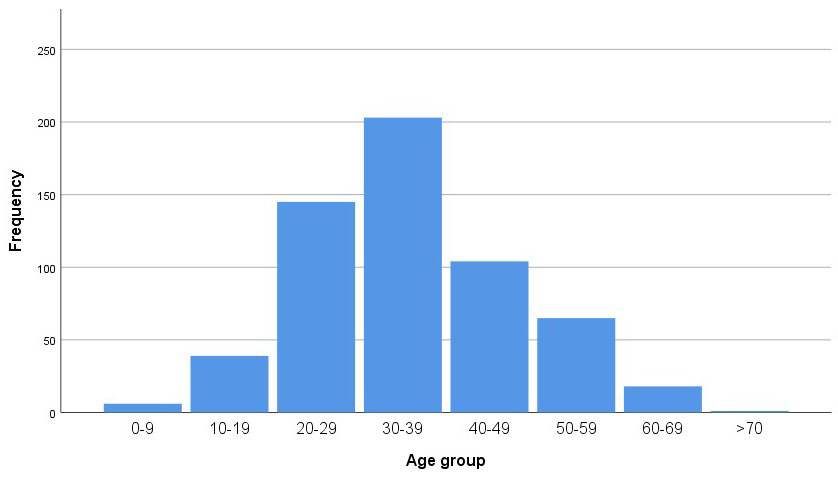
A total of 8,412 biopsies were received by the department and processed for histopathologic diagnosis in the five-year period between 2015 and 2020. Out of these, 581 (6.9%) were thyroid tissue specimens. Female patients constituted 468 (80.6%) of the total thyroid cases. The age distributions have minimum value of 3-years and a maximum value of 70-years with mean age of 34.8 a and the standard deviation of 11.4 (Figure 1). The most commonly affected age group with thyroid lesions was between ages 30 and 59 (88.9%). Most of the patients, 353 (60.8%), were from surrounding areas with variable distance from Jimma town, while 208 (35.8%) patients were from Jimma town (Table 1).
Figure 1. Demographic Characteristics of Thyroid Lesions, 2015-2020, JMC, Jimma, Ethiopia
| Table 1. Demographic Characteristics of Thyroid Lesions, 2015-2020, JMC, Jimma, Ethiopia |
| |
|
Sex
|
Total
|
| |
|
Male
|
Female
|
|
Age groups
|
<18
|
5 |
14 |
19
|
|
18-30
|
36 |
135 |
171
|
|
30-60
|
65 |
307 |
372
|
|
> 60
|
7 |
12 |
19
|
|
Place of residence
|
Surrounding area |
51 |
302 |
353 |
| Jimma town |
55 |
153 |
208
|
Clinical Presentation
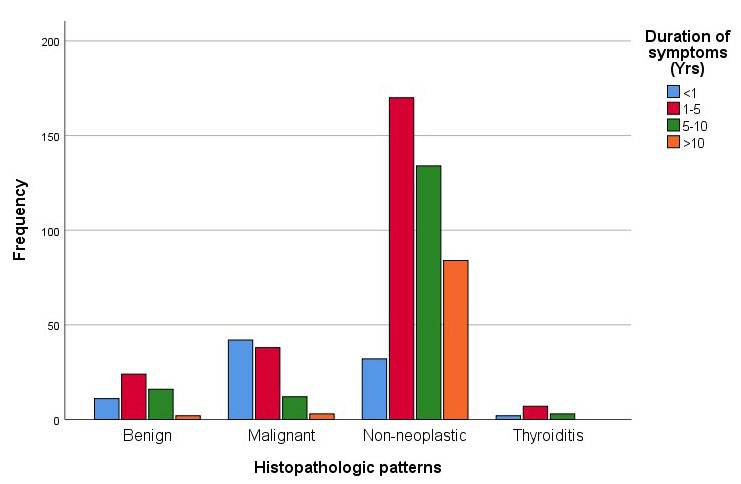
Most patients (41.2%) presented with a history of 1-5-years duration. The majority of malignant tumours, constituting about 42 (44.2%) cases present with relatively short duration of symptoms (<1-year) (Figure 2).
Figure 2. Bar Graph Showing Duration of Symptoms and Histopathologic Patterns of Thyroid Lesions, 2015-2020, JMC, Jimma, Ethiopia
Histopathologic Patterns of Thyroid Lesions
Nonneoplastic lesions were encountered in 432 (74.3%) cases in which nodular colloid goitre (NCG) predominates. Among the nonneoplastic cases, 417 (71.8%) were NCG and the remaining 3 cases were thyroglossal duct cysts (Table 2). Thyroiditis constituted 12 (2.1%) of the cases. Thyroid neoplasms were encountered in 149 (25.6%) cases. Benign neoplasms i.e., adenomas were seen in 54 (9.3%) cases and include follicular adenoma, hurthle cell adenoma and non-invasive follicular thyroid neoplasm with papillary like nuclear features (NIFTP) (Table 3).
| Table 2. Categories of Histopathologic Patterns of Thyroid Lesions and their Frequencies, 2015-20, JMC, Jimma, Ethiopia |
|
Histopathologic Diagnosis
|
Frequency |
Percentage (%)
|
| Non-neoplastic |
420
|
72.3
|
| Thyroiditis |
12
|
2.1
|
| Benign neoplasms |
54 |
9.3
|
| Malignant neoplasms |
95
|
16.3
|
| Total |
581
|
100
|
| Table 3. GHistopathological Patterns of Thyroid Lesions Encountered in Thyroid Biopsy Specimens, 2015-20, JMC, Jimma, Ethiopia |
|
Age Group
|
Group B |
Total
|
| NCG |
417
|
71.8
|
| Papillary thyroid carcinoma |
69
|
11.9
|
| Follicular adenoma |
42
|
7.2
|
| Follicular carcinoma |
14
|
2.4
|
| Lymphocytic thyroiditis |
8
|
1.4
|
| Hurthle cell adenoma |
7
|
1.2
|
| Hurthle cell carcinoma |
6
|
1.0
|
| NIFTP* |
4
|
0.7 |
|
Subacute thyroiditis
|
4 |
0.7
|
| Medullary carcinoma |
3
|
0.5
|
|
Thyroglossal duct cyst
|
3 |
0.5
|
| Poorly differentiated carcinoma |
2
|
0.3
|
| Anaplastic carcinoma |
1
|
0.2
|
| WDTUMP** |
1
|
0.2
|
| Total |
581
|
100.0
|
| *NIFTP-Non-invasive follicular thyroid neoplasm with papillary like nuclear features **WDTUMP- Well differentiated tumour of uncertain malignant potential |
Most of the non-neoplastic thyroid lesions are seen between the ages of 30-39, which is the commonest age group seen at presentation (Table 4). Among different histopathologic patterns, 468 cases are seen in females with a female to male ratio of 4.1:1.
| Table 4. Distribution of Histopathological Patterns of Thyroid Lesions with Age 2015-2020, JMC, Jimma, Ethiopia |
| |
|
Histopathologic Patterns
|
Total
|
| |
|
Benign
|
Malignant |
Non-neoplastic |
Thyroiditis
|
| Age group |
0-9
|
– |
2 |
4 |
– |
6
|
|
10-19
|
6 |
5 |
28 |
– |
39
|
|
20-29
|
20 |
26 |
94 |
5 |
145
|
|
30-39
|
19 |
21 |
161 |
2 |
203
|
|
40-49
|
6 |
21 |
75 |
2 |
104
|
|
50-59
|
2 |
11 |
49 |
3 |
65
|
|
60-69
|
1 |
8 |
9 |
– |
18
|
|
>70
|
– |
1 |
– |
– |
1
|
| |
|
54
|
95 |
420 |
12 |
581 |
Thyroiditis represents twelve (2.1%) of the cases with female to male ratio of 5:1 and a mean age at presentation of 34.8+11.4. Eight (66.6%) of the cases were chronic lymphocytic thyroiditis/Hashimoto’s thyroiditis whereas the rest of four cases were subacute thyroiditis.
Fifty-four (54) benign neoplasms were diagnosed in the time period, which accounts for 9.3% of all cases. The most common benign neoplasm was follicular adenoma 42 (77.7%) with a female to male ratio of 5:1 followed by hurthle cell adenoma 7 (12.9%) and only 5 cases of NIFTP were diagnosed (9%). They were mostly diagnosed in the age group 20-39 in 72.2% of the time with average age of 34.8 and standard deviation (SD) of 11.5.
The most common morphologic subtype of carcinoma was papillary thyroid carcinoma which accounts for 69 (72.6%) of the total 95 cases with a female to male ratio of 2.8:1 followed by follicular carcinoma 14 (14.7%) and hurthle cell carcinoma 6 (6.3%) (Table 5). Regarding the age distribution of malignant thyroid tumours, most of the diagnosis is made in the 20-49 age group in 71.6% of cases with an average age of 34.8 and SD of 11.5.
| Table 5. Histopathological Subtypes of Thyroid Carcinoma, 2015-20, JMC, Jimma, Ethiopia |
|
Thyroid Carcinoma
|
No. |
%
|
| Papillary thyroid carcinoma |
69
|
72.6
|
| Follicular carcinoma |
14
|
14.7
|
| Hurthle cell carcinoma |
6
|
6.3
|
| Medullary carcinoma |
3
|
3.2
|
| PDTC |
2
|
2.2
|
| Anaplastic carcinoma |
1
|
1
|
| Total |
95
|
100
|
Association of Thyroid Lesions with other Variables
Age (p=0.010), sex (p=0. 016), place of residence (p=0.177) and duration of symptoms (p=0.00) were tested at p<0.05 for their association and selected as candidate variables for binary logistic regression. Binary logistic regression analysis was performed in backward method with a likelihood ratio through two steps and two blocks on these variables and finally, age (p=0.004) and duration of symptoms (p=0.000) were showed to be the independent predictors of benign and malignant thyroid lesions, which was statistically significant as shown on the table. However, there was no statistically significant association between place of residence and thyroid lesions (p=0.144) (Table 6).
| Table 6. Binary Logistic Regression of Thyroid Lesions and Associated Factors, 2015-2020, JMC, Jimma, Ethiopia |
|
Variables in the Equation
|
B |
S.E. |
Wald |
df |
Sig. |
Exp(B)
|
|
Step 1a
|
Age group
|
0.708 |
0.254 |
7.768 |
1 |
0.005 |
2.029
|
|
Residence
|
-0.390 |
0.267 |
2.137 |
1 |
0.144 |
0.677
|
|
Duration of symptoms
|
-2.049 |
0.269 |
58.109 |
1 |
0.000 |
0.129
|
|
Sex
|
-0.603 |
0.293 |
4.236 |
1 |
0.040 |
0.547 |
| Constant |
2.647 |
0.879 |
9.062 |
1 |
0.003 |
14.117
|
|
Step 2a
|
Age group
|
0.723 |
0.253 |
8.154 |
1 |
0.004 |
2.060
|
|
Duration of symptoms
|
-2.038 |
0.268 |
57.946 |
1 |
0.000 |
0.130
|
|
Sex
|
-0.525 |
0.288 |
3.320 |
1 |
0.068 |
0.592
|
|
Constant
|
1.943 |
0.728 |
7.124 |
1 |
0.008 |
6.983
|
| a Variable(s) entered on step 1: age group, residence, duration of symptoms, sex. |
Thyroid cancer was found to be more common in females than males with a female to male ratio of 2.6:1. However, there was a statistically significant association between male sex and incidence of thyroid malignancy (p=0.040). Based on histopathology results, of the 113 male patients operated for thyroid lesions at JMC during the study period, twenty-six (23%) were diagnosed with thyroid malignancy (18 with papillary thyroid cancer (PTC), 5 with Follicular carcinoma, 2 with hurthle cell carcinoma and 1 with poorly differentiated thyroid cancer (PDTC)). In contrast, only 14.7% (69/95) of the women were diagnosed with thyroid cancer. Hence, the odds of being diagnosed with thyroid
cancer is 1.7 times higher in males than females (p-value of 0.033, adjusted odds ratio (AOR) of 1.73, and 95% CI (1.05-2.3).
Cyto-Histologic Correlation
A total of 286 FNAC results which were done prior to undergoing thyroidectomy were retrieved and correlated with the corresponding final histopathologic diagnosis. They were grouped according to the Bethesda system of reporting for thyroid cytology into five groups (Table 7). Only two (0.7%) were nondiagnostic/unsatisfactory for evaluation. In these two cases, one turned out to be Thyroglossal duct cyst and the other NCG with the final histopathologic diagnosis. There were 225 female and 61 male patients with a female to male ratio of 3.7:1 with a mean age of 34.8.
| Table 7. Cross Tabulation Showing Correlation of FNAC and Histopathologic Diagnosis, 2015-2020, JMC, Jimma, Ethiopia |
| |
|
Histopathologic Patterns
|
Total
|
| |
|
Benign
|
Malignant |
Non-neoplastic |
Thyroiditis
|
|
FNAC diagnosis
|
Non-diagnostic
|
0 |
0 |
2 |
0 |
2
|
|
Benign/NCG
|
22 |
22 |
157 |
2 |
203
|
|
SFN/FN/HN/SFHN*
|
23 |
18 |
9 |
1 |
51
|
|
Suspicious for malignancy
|
1 |
7 |
7 |
0 |
15
|
|
Malignant
|
1 |
10 |
4 |
0 |
15
|
|
Total
|
|
47
|
57 |
179 |
3 |
286
|
| *SFN/FN/HN/SFHN- Suspicious for follicular neoplasm, follicular neoplasm, Hurthle cell neoplasm, Suspicious for huthle cell neoplasm respectively |
Fifteen cases were categorized as suspicious (i.e., indeterminate). Seven (46.7%) of the fifteen cases corresponded histologically as carcinoma (Papillary thyroid carcinoma). Seven (46.7%) cases turned out to be non-neoplastic (NCG) and one case was follicular adenoma.
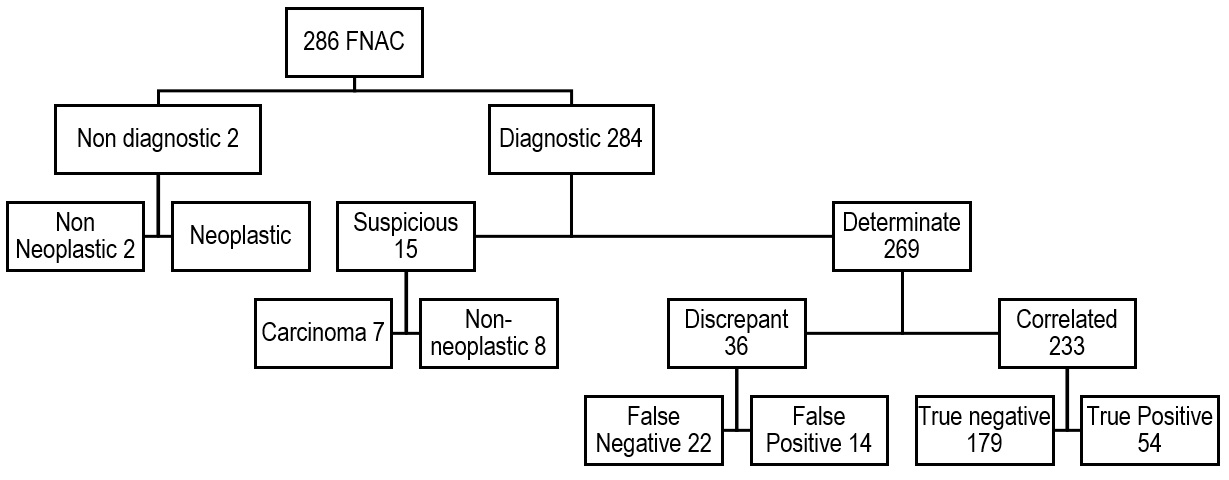
Two hundred sixty-nine (269) Aspirations (94.1%) were diagnostic (determinate). When compared with their corresponding histopathologic diagnosis, 36 (13.4%) of the cases were discrepant (22 false negatives and 14 false positives). However, 233 (86.6%) cases were correlated with histopathologic diagnosis (179 true negative and 54 true positive). The false negative rate was 8.2% and the false positive rate was 5.2%. The overall sensitivity and specificity for cytologic diagnosis was 71% and 92.7% respectively. The accuracy of FNAC in this series is 86.6%. The Negative predictive value was 89.1%.
All of the 22 false negative cases, were diagnosed as NCG and the corresponding histopathologic examination turned out to be papillary thyroid carcinomas in 16 cases, 5 cases were follicular carcinoma and 1 was hurthle cell carcinoma.
Among 14 false positive cases 10 cases were diagnosed as follicular patterned lesions (follicular neoplasm/suspicious for follicular neoplasm/hurthle cell neoplasm/suspicious for hurthle cell neoplasm) and upon confirmation with histopathology, 9 cases were NCG and 1 case was lymphocytic thyroiditis. The remaining 4 cases were diagnosed as Papillary thyroid carcinoma by cytology but were colloid goitre histologically. The overall cytohistologic correlation results are summarized in Table 8 and Figure 3.
| Table 8. Summary of FNAC Results, 2015-2020, JMC, Jimma, Ethiopia |
|
Summary of 286 FNAC Results
|
%
|
| Non-diagnostic |
0.7%
|
| False negative |
8.2%
|
| False positive |
5.2%
|
| Sensitivity |
71%
|
| Specificity |
92.7%
|
| Accuracy |
86.6%
|
Figure 3. Diagram Showing Cyto-histologic Correlation of 286 FNAC Results, 2015-2020, JMC, Jimma, Ethiopia
DISCUSSION
The age group commonly affected with thyroid lesions in this study is, 20-59 which accounts for 88.9% of the cases with an average age of 34.8. This is in agreement with a study done in Tikur Anbesa Hospital, Ethiopia, in which 85% of the patients with thyroid lesion fall under the age group 20-59.7 Diseases of the thyroid are more common in women with female to male ratio of 4.1:1 with 468 (80.6%) cases seen in females. This is consistent with studies done in Kenya, Nigeria and Saudi Arabia with variable ratios reflecting different study populations.8,9,10 High ratio of thyroid lesions in the female sex was suggested to be from a level of hormonal variation after puberty and this study does seem to validate this scientific explanation.11
Non-neoplastic thyroid lesions constitute 432 (74.3%) of overall cases. NCG by itself accounts for 417 (71.8%) of overall thyroid lesions. This is consistent with a study done in St. Paul’s Hospital Millennium Medical College (SPHMMC) (Addis Ababa, Ethiopia) in which 152 (68.4%) of the cases were NCG.12 This picture is also found to be a consistent finding when compared to similar studies done in Uganda that showed NCG to be the commonest consisting of 90 (65.7%), Yemen 164 (63.1%) and Bangladesh 81 (75%) of the cases.8,13,14
Thyroiditis is seen in twelve (2.1%) of the cases with a female to male ratio of 5:1 and a mean age at presentation of 34.8+11.4 with 8/581 (1.3%) of the overall thyroid lesions being chronic lymphocytic thyroiditis/Hashimotos thyroiditis. Two studies done in India show the frequency of Lymphocytic thyroiditis at 30 (2%) and 37 (1%) with a mean age of 40+10 which is in agreement with this study.15,16 A study done in Italy also shows the frequency to be 54 (1.4%) of the cases.17
Neoplastic diseases of the thyroid were found to be 149 (25.6%) constituting the second most common thyroid lesion in the study with female to male ratio of 5:1. Benign neoplasms were seen in 54 (9.3%) of the cases with follicular adenoma being the most common, 42 (77.8%) followed by 7 cases of hurthle cell adenoma (12.9%), NIFTP 5 cases (9.3%) and 1 case (1.8%) of well differentiated tumour of uncertain malignant potential (WDTUMP). This figure is comparable with similar study conducted by Tsegaye et al7 in Addis Ababa in which 164 (21%) were thyroid neoplasms in which 100 (60.9%) were adenomas. Study done in Western Kenya indicates occurrence of benign neoplasms to be 51 (13.1%) which is comparable with this study.18 A retrospective study done in Southern Nigeria shows frequency of 36 (12.1%) benign neoplasms with similar female to male ratio of 5:1, with follicular adenoma constituting thirty-three (91%) of the cases.19 A slight variation in the frequencies can be due to different sample sizes and duration of the study. A similar study done in Pakistan shows a total of 255 (26%) neoplastic lesions, which is consistent with the current study. However, among the benign neoplasms follicular adenomas account for 67 (65.9%) cases, which is lower than the figure seen in the current study.20 This can be explained by the strict histopathologic criteria employed in the study in classifying benign thyroid neoplasms in the aforementioned study which was technically difficult to employ in the current study.
Among the 581 biopsies, ninety-five (16.4% of total cases and 63.8% of all thyroid neoplasms), cases were malignant with a female to male ratio of 2.65: 1 and most are seen in the age group 20-29 accounting for 26 (27.4%) of cases. There is an overall predominance of malignant thyroid neoplasms over the benign counterparts in this study. As the study hospital is the largest tertiary referral hospital in the southwestern part of the country, most cases are referral cases with suspected malignancy. This can contribute to the higher incidence of cancers in the hospital, and this is also a reflection of the increasing prevalence of thyroid cancer in the region and mandates larger scale studies to determine the underlying causes and associated factors. However, such figures are also seen in other studies across the continent.10,20,21
Among the malignant thyroid neoplasms, Papillary thyroid carcinoma was the most common with a frequency of sixty-nine (72.6%) cases with a female to male ratio of 2.8:1, mean age at presentation of 35.6 and 30 (78.9%) cases have a 1-5-year history of symptoms. This figure is similar with the study conducted in Tikur Anbesa hospital which shows 49 (76.9%) cases to be papillary thyroid carcinomas.7 Similar predominances of papillary thyroid carcinoma is reported in other literatures with variable proportions.22-25 Papillary thyroid carcinoma was the most common malignancy in study done in Nigeria which accounts for 98 (56.3%) cases with peak incidence in the 3rd decade.9 Another study done in Saudi Arabia shows papillary thyroid carcinoma to be the most common malignancy accounting for 105 (74%) of cases with mean age of 37.5-years.26 Study conducted in Ireland from consecutive 1,003 thyroidectomy specimens 261 were malignant in which papillary carcinoma accounted for 75.1% of cases.8 Large scale study in Sao Paulo, Brazil, which shows 9,607 (72%) cases of papillary carcinoma and similar study done in United States of America (USA) shows 28,414 (86%) cases.24
Only fourteen (14.7%) cases of follicular carcinoma were seen in this study with mean age of 36.9 and presenting within 1-year of development of symptoms in 8 (57.4%) cases. This is in agreement with study conducted in Gondar city in which eighteen (29%) of the cases turned out to be follicular.27 However, this is contrary to the finding of a study done in Harare, Zimbabwe, in which follicular carcinoma was the most common malignancy seen in 60 (70%) patients.25 This shows that follicular carcinomas may be a reflection of a more severe iodine lack in certain populations or indeed a reflection of some etiological differences for this tumour in the different populations.
Medullary carcinoma is still relatively uncommon with only three (0.5%) cases identified in this study, which is in agreement with findings from two studies in Addis Ababa in which only one and two cases were found, Port-Harcourt, Nigeria (one case), Yemen (two cases) as well as reports from Pakistan (four cases).7,14,20,28 Only one case of Anaplastic thyroid carcinoma was identified in this study (A 70-year-old male patient) which is in harmony with other reports of rare incidence of this disease entity.21,22,24,29
Diagnostic sensitivity and specificity of FNAC in this study are 71% and 92.7% respectively. These figures are slightly higher than similar study done by W. Ergete and D. Abebe in which the sensitivity and specificity were 67% and 84.7% respectively.30 Similar studies done in Tanzania show 66.7% sensitivity and 92.5% specificity.31 Even lower sensitivity of FNAC (61.5%) in diagnosing malignancy is reported in Uganda.32 This is also in harmony with other studies in which in areas with a high prevalence of multinodular goitre, the sensitivity for detecting malignancy is relatively low whereas specificity is high.33
Among 286, FNAC’s cyto-histologic correlation was achieved in 233 (86.6%) cases. Such concordance rate is in agreement with a study done at Tikur Anbesa Hospital in which 274 cases (82%) were correlated.30 Similarly, a correlation study conducted in the USA shows an 88% correlation.33
False negative and false positive results account for 22 (8.2%) and 14 (5.2%) respectively. This is in agreement with an Egyptian study in which the false negative and false positive rates were 7.2% and 5.8 % respectively.4 Similar figures are also seen in a study conducted to determine discordance rate between thyroid cytology and histopathology in the USA in which 8% false negative and 4% false positive results were found.33 The overall reported false negative rates range from 1-11%. According to various literatures it is difficult to establish the true frequency of false-negative results, since only a small percentage (approximately 10%) of patients with benign cytologic findings undergo surgery. However, all reports agree that if all patients with thyroid fine needle aspiration (FNA) also had histologic examinations, the true false-negative rate would be below 5%.6,`34,35
Diagnostic accuracy of FNAC in this study was 86.6% with a negative predictive value (NPV) of 89.1% and a positive predictive value (PPV) of 80%. Accuracy is slightly higher than a study done in Tikur Anbesa Hospital which shows 82% diagnostic accuracy.30 A Study done in Tanzania to assess the cytohistologic correlation of thyroid lesions shows accuracy of 81.4% with NPV of 86% and PPV of 75%.31 Similar study conducted in Uganda shows diagnostic accuracy, NPV and PPV of 85.9%, 93.9% and 47% respectively.32 Study done in USA shows diagnostic accuracy of FNAC to be 86.8% with NPV and PPV of 90% and 85.4% respectively.33
With regard to the risk of malignancy in suspicious or indeterminate groups, seven out of fifteen suspicious cases (46.7%) correlated with histopathologic diagnosis of thyroid carcinoma. Thus, there is a significant probability that a cytologically indeterminate lesion could be neoplastic, and there is a good chance that this lesion will be malignant. This is in agreement with a study done in Tikur Anbesa Hospital showing four out of seven suspicious cases (57%) turning out to be malignant and a study done in the USA in which 19 out of 40 suspicious cases (47%) were indeed malignant.30,33
CONCLUSION
Neoplastic thyroid diseases are not rare entities and thyroid malignancy is found to be more common than benign neoplasms. This study also shows cyto-histologic correlation of 86.6% with overall sensitivity and specificity of FNAC 71% and 92.7% respectively. The diagnostic accuracy of FNAC was found to be 86.6%. FNAC remains to be an important diagnostic tool. These findings also give good preliminary data on the performance of FNAC in our setting.
ETHICAL CONSIDERATION
Ethical clearance was obtained from Institutional Review Board of Jimma University and was submitted to the responsible authorities of JMC department of Pathology before proceeding to data collection. All the information collected from the study was handled confidentially.
CONFLICTS OF INTEREST
The authors declare that they have no conflicts of interest.


