INTRODUCTION
At present, there is a dramatic rise in the incidence of diabetes all over the world. Under 3% of the absolute infection, each of diabetes, asthma, and hypertension has been accounted for among Hajjis amid the time of Hajj.1 The exact inheritance pattern of this condition as for whether it is transmitted through the paternal side or maternal side is not found. Family history has been considered as one of the risk factors of diabetes.2 Congregation of information on family history of the disorder for assessing the risk has been used very less in the practice of preventive medicine and early detection.3In order to encourage change in lifestyle and initiate interventions of the condition, medical guidelines mostly include family history as the use of this tool was more advantageous over other genomic tools.4 In India, the studies regarding the effect of positive family history of diabetes are still required.2
The inheritance pattern of type 2 diabetes is quite complex to understand because many other factors are also affecting this habits, such as lifestyle patterns, physical activity status, dietary propensities and so forth the ecological components. These complex relationships between genetic factors and environmental conditions may be reflected by tracing family history.5 Till date, molecular genetics could not find out successfully the genetic markers of this condition.6 Type 2 diabetes is known to be a heritable condition but no specific gene has been found for the common form of diabetes.6,7 The relative contributions of paternal and maternal influences could provide information about the parental effects on their children and hence study of the parental transmission of diabetes would be very valuable.8 In the present study, we have endeavored to find out whether the transmission of diabetes is higher from the paternal side or from the maternal side. In fact, it will be helpful in understanding the disease more deeply.
METHODS
The study was conducted in Manipur among the Muslim communities of two districts. Four hundred participants of each gender were actively involved in the study, out of which 200 were patients with diabetes and 200 had no diabetes. The purpose of the study was properly explained to the participants before starting the work in order to make them understand and aware of it. Those who gave written consent were only included in the study. The active participants with diabetes in this study were under medical supervision. Ethical approval was taken from the Institutional Ethical Committee before the fieldwork was carried out.
Standardized proforma was used in order to gather the required information. Socio-demographic data were also collected. Genealogies of the participants were drawn for the purpose of tracing the inheritance pattern of the disease. Only those participants who were well understood for the family history of the disease were studied in the present study. The others were not considered for genealogical tracing. Age at onset of diabetes was also recorded for each participant. Basic anthropometric measurements were taken by using anthropometer and weighing machine using the standardized procedure. The data collected were analyzed by using SPSS 17.0 version and interpreted.
RESULTS AND DISCUSSION
The demographic data of the present study is displayed in table 1. Table 1 shows sex-wise distribution the mean and standard deviation of age (self), age of spouse, age at marriage (self) and spouse age at marriage along with its t-values. Mean age of males with diabetes were found to be older than females with diabetes. Mean age of spouse and age at marriage of spouse were younger among males as compared to females with highly significant t-value (p<0.001). Age at diagnosing diabetes was lower among females.
| Table 1. Age of Participants with Diabetes |
|
Age in years
|
Mean ± Standard Deviation |
| Male |
Female |
t-value
|
| Age self |
41.2±4.16
|
40.6±4.79 |
0.945
|
| Age of spouse |
35.4±10.22
|
42.7±14.22 |
-4.207***
|
| Age at marriage (self) |
21.5±6.99
|
19.2±4.87 |
2.698
|
| Age at marriage of spouse |
18.2±6.14
|
25.0±6.09 |
-7.870***
|
| Age at diagnosing diabetes |
36.1±5.39
|
35.50±5.292 |
0.820
|
| ***p<0.001 |
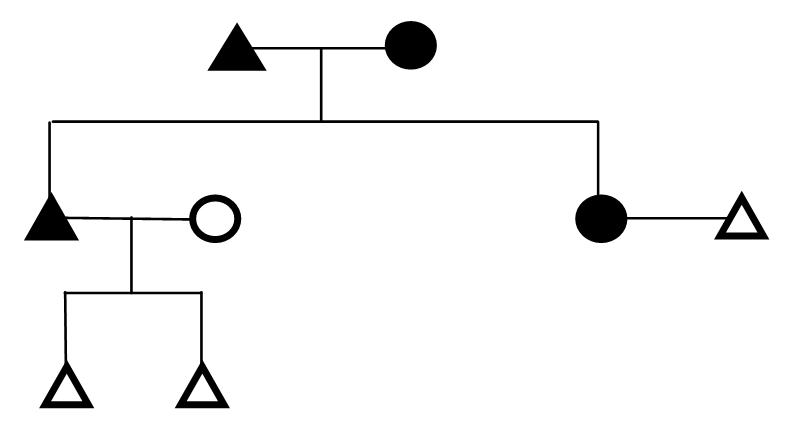
Figure 1 indicates the distribution of participants according to different inheritance pattern of families with diabetes. This result was found from the analysis of genealogy of 93 families from the present study. Three different diagrams A, B and C were shown in order to demonstrate the transmission pattern. On comparing figure 1A and 1B maximum percentage of transmission of diabetes to son, daughter and both son and daughter was found to be from the paternal side. Additionally, figure 1C represents the contribution of both maternal and paternal side in the transmission of diabetes to their children. The different inheritance patterns of the disease were displayed distinctly by genealogical representation figures 2-10.
Figure 1(A, B, C). Distribution of Participants of 93 Families with their Inheritance Pattern
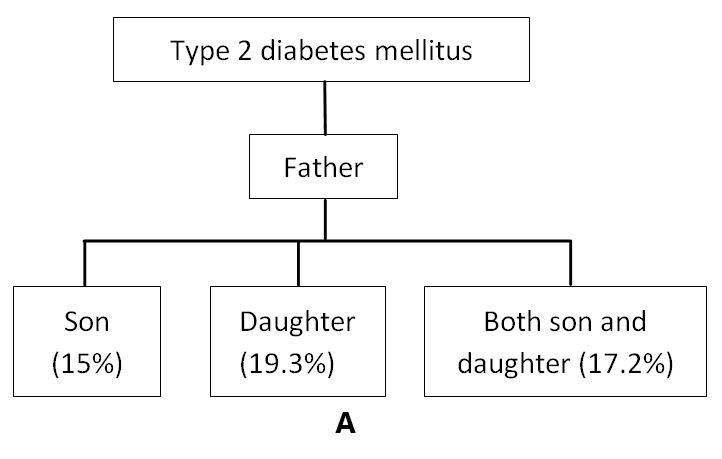
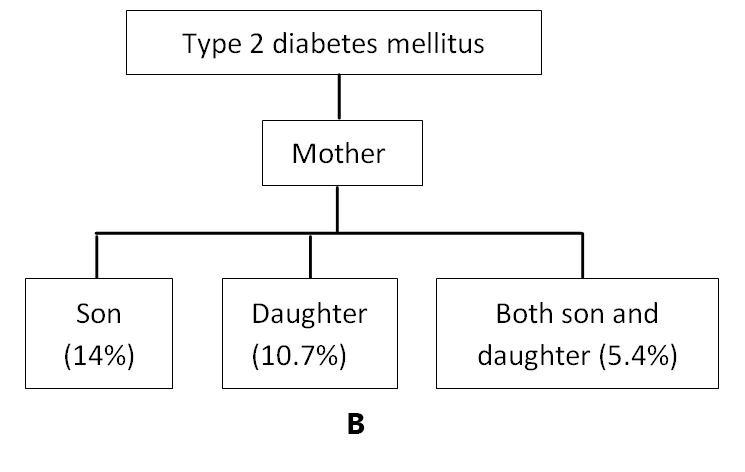
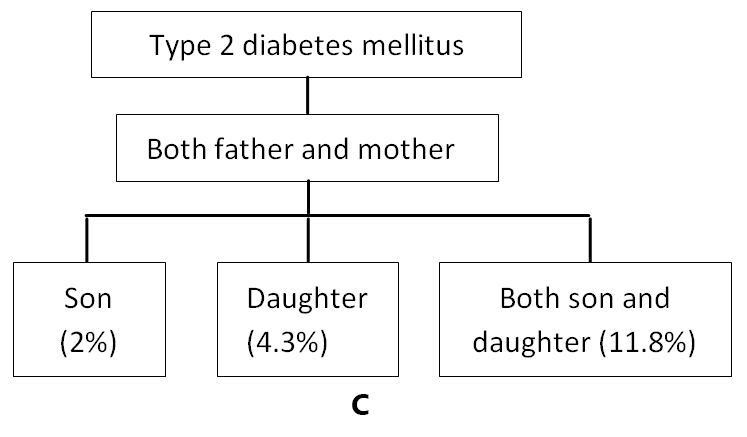
Figure 2. Genealogical Representation of a Family Showing Father with Diabetes and Inheritance Pattern of Disease to Son
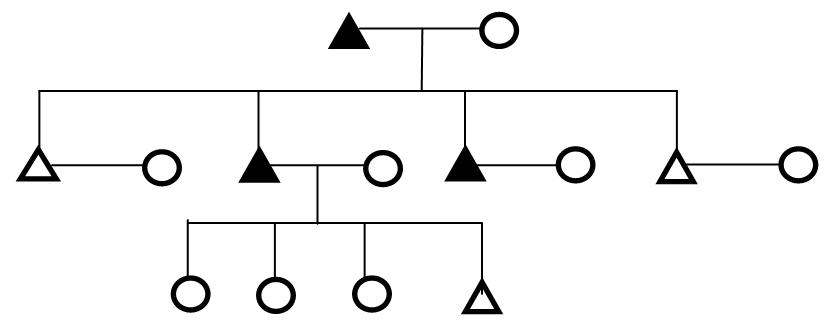
Figure 3. Genealogical Representation of a Family Showing Mother with Diabetes and Inheritance Pattern of Disease to Son
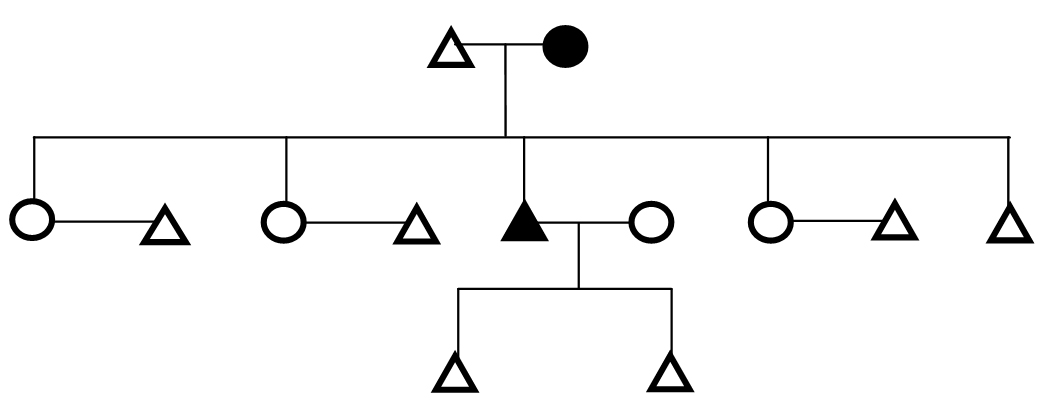
Figure 4. Genealogical Representation of a Family Showing Both Parents with Diabetes and Inheritance Pattern of Disease to Son
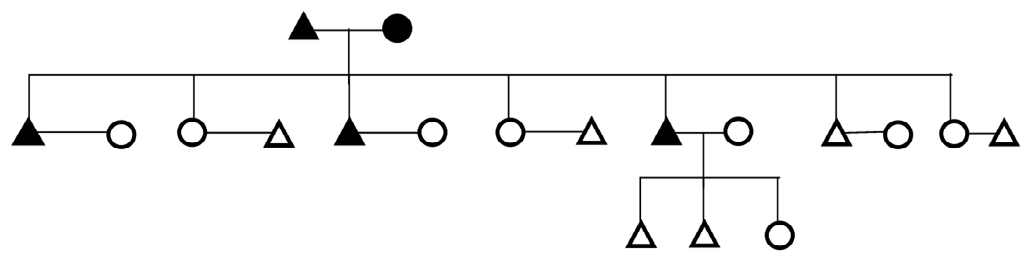
Figure 5. Genealogical Representation of a Family Showing Father with Diabetes and Inheritance Pattern of Disease to Daughter
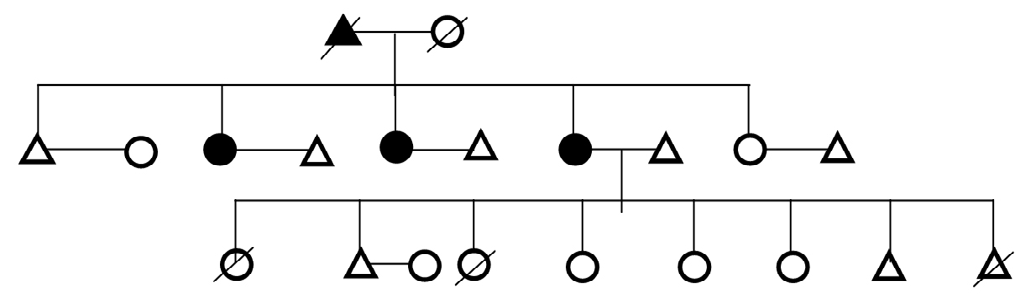
Figure 6. Genealogical Representation of a Family Showing Mother with Diabetes and Inheritance Pattern of Disease to Son
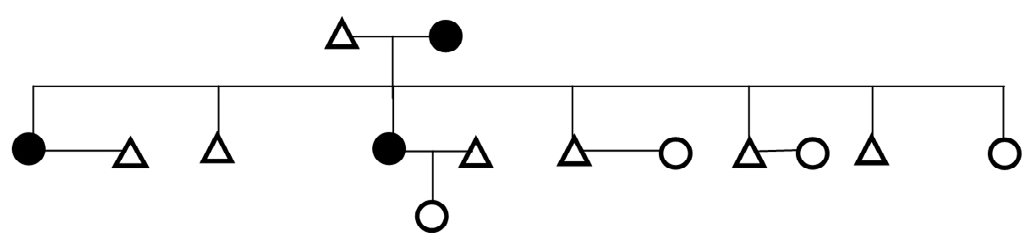
Figure 7. Genealogical Representation of a Family Showing both Parents with Diabetes and Inheritance Pattern of Disease to Daughter
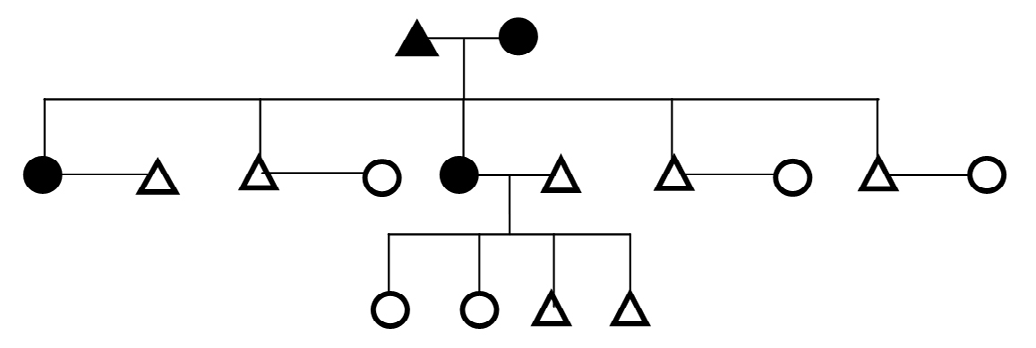
Figure 8. Genealogical Representation of a Family Showing Mother with Diabetes and Inheritance Pattern of Disease to Both Son and Daughter
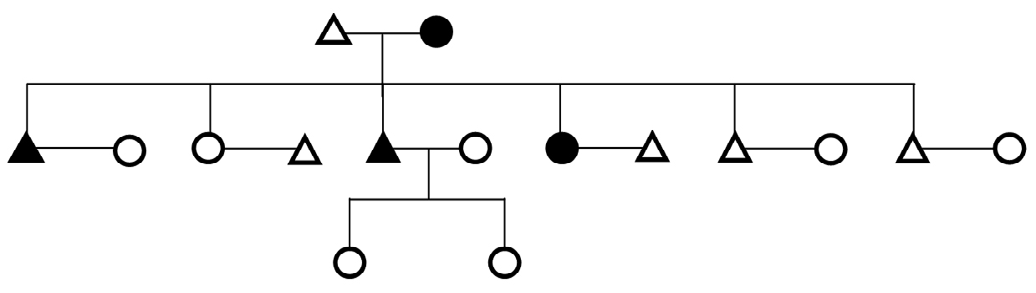
Figure 9. Genealogical Representation of a Family Showing Father with Diabetes and Inheritance Pattern of Disease to Both Son and Daughter
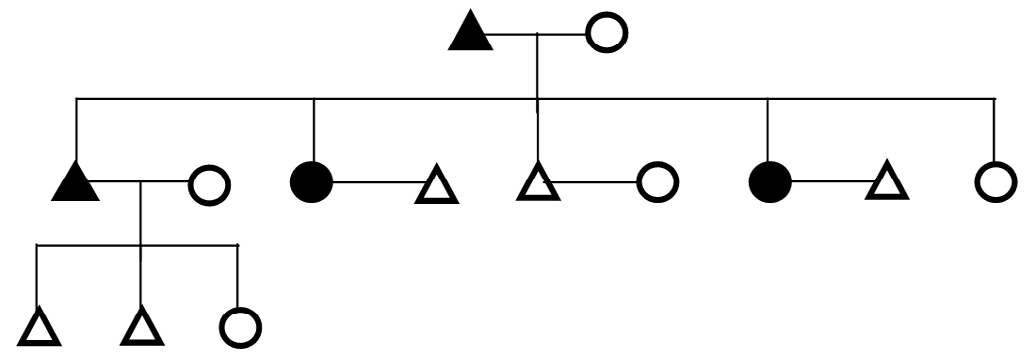
Figure 10. Genealogical Representation of a Family Showing Parents with Diabetes and Inheritance Pattern of Disease to Both Son and Daughter
Voluminous amount of research has been done on this major burden of the disease since many years in the past and are continuing till today among different ethnic groups of different regions for finding out the useful results that would help in decreasing the worldwide prevalence. Large numbers of people in India i.e. around 41 million have diabetes and it is expected to rise to 70 million in 2025. India being the second most populous country in the world has a wide diversity in terms of caste, religion, habitat, food habits, lifestyle, and financial status.9
The present study demonstrated that the mean age of self and age of spouse of the participants were older than the participants without diabetes. Mean of self-age at marriage and age at marriage of the spouse was lower among participants without diabetes as compared to the participants with diabetes. In addition to these, the mean of age at diagnosing diabetes was early among the female participants with diabetes as compared to their male counterparts. It showed consistency with the earlier study by.10 The reason for the early onset of diabetes among the females might be due to the lesser activity level of the body as most of the females stayed at home and after completing their household chores, they spent their leisure times on watching TV for long duration or slept during the daytime. Due to a sedentary lifestyle, early onset of diabetes among them could be explained as one of the reason.
In the present study, it was found that highest percentage of participants with diabetes of both sexes were married as compared to participants without diabetes and also showed significant differences. Some societies were found to have relationship of diabetes with single or married individuals.11 Marriage may increase the stress level of an individual for providing for the family12 which may further result in the reduction of activation of the neuroendocrine system. Information about diabetes in the north east region including the present study area, Manipur was very less.13
On tracing the genealogies of different families with diabetes in the present study, paternal transmission of the disease was found to be in the highest percentage. The transmission was not only to either son or daughter but to both sexes. It was supported by the research6 on a randomly selected community of Framingham in which it was found that unique paternal genetic factors might transmit diabetes to children.6 This also reported the risk of this disease to be 3.5 fold higher among offspring with only one parent with diabetes while it was 7 times higher with two parents with diabetes as compared to the offspring of parents without diabetes.
The present study suggested the contributions of the paternal role of the disease. The reason for this might be due to both father and mother genes were accountable in forming an offspring. In addition to this, those genes contributed by father might possess the factors affecting the disease before exposure to the uterine environment of the mother. In a study conducted by McCarthy et al14 on a south Indian population in London, maternal history was more common as compared to the paternal history and it was not significant. However, the finding that excessive maternal transmission of diabetes15 was not supported by the recent study and also by another previous study by Thorand et al.16
CONCLUSION
Both paternal and maternal factors might be responsible for the transmission of diabetes. The present study among the Muslims of Manipur found paternal inheritance of diabetes to be higher in percentage on tracing the genealogy of families with diabetes. This study would provide expedient information to the forthcoming researchers as well as to the common people in understanding the disease. Further, more researches are needed to be carried out among different communities of diverse regions for assessment and also to elucidate whether ethnicity plays a role or not on the transmission of diabetes.
ACKNOWLEDGEMENTS
The authors are grateful to the participants of the two districts of Manipur for their immense support and corporation during the study. This work was supported by Delhi University – University Grant Commission non-net fellowship to NF, SK and MD by R &D, DU. NF designed the study, collected, analysed and drafted the manuscript. MD directed implementation and provided necessary logistical support and SK edited the manuscript and provided critical comments.
CONFLICT OF INTEREST
The authors declare that they have no conflicts of interest.


