INTRODUCTION
Vulvovaginal atrophy is a common condition in post-menopausal women but underreported especially in the Indian subcontinent probably due to the lack of awareness, inaccessibility to the appropriate treatment and stigma. Nearly 50% women suffer from varying symptoms and these may include dryness, irritation, soreness and dyspareunia with urinary frequency, urgency and urge incontinence.1
Decreased estrogenization of the vaginal tissue leading to thinning of the vaginal mucosal epithelia is the main underlying pathology owing to atrophy of the vaginal wall which contributes to the cardinal symptom of vaginal dryness.2 Clinically, the vagina may appear pale and at times small multiple petechiae may be noted. This in turn can also harbor different pathogens causing recurrent urinary tract infections. The decline in genital and sexual health can be quite detrimental and adversely affect the quality of life (QoL).3
Current therapeutic approaches include topical treatments and hormones. Non-hormonal therapies which include vaginal moisturizers and lubricants provide relief for mild symptoms, while estrogen therapy is the most effective treatment for moderate to severe symptoms. They have to be used regularly for long-term to achieve desirable effects.4 However, endometrial safety has not been studied in long-term clinical studies, and there are insufficient data to confirm the safety of local estrogen in women with breast cancer.5 Hormone replacement therapies are also tried which has poor patient compliance and many of the times not that effective.6 Surgeries are performed by gynaecologists and plastic surgeons on to the pelvic floor but not every patient may be suitable considering post-operative complications and downtime.6 Hence the choice of therapy remains controversial as it is mainly based on the severity of symptoms, safety and ultimately, patient preference.4
The recent innovation of energy based devices has brought in a whole new array of treatment modalities with more promising results. Among these devices, fractional carbon dioxide (CO2) laser has gathered a lot of attention due to its far superior ability to demonstrate significant improvement in vulvovaginal atrophy (VVA) patients. It has the advantage of being non-invasive with minimal or no down time, painless and has a better outcome.7
Laser CO2 which has already gained popularity in dermatologic and esthetic surgery uses a wavelength (10,600 Hz) having high water absorption which could ablate and coagulate vaginal and vulvar tissues. This stimulates neocollagenesis, and neovascularization and thus improves vaginal lubrication by revitalizing and restoring the elasticity and hydration of the female lower genital tract mucosa.8
There have been no published trials on Indian women so far with respects to the use of fractional CO2 laser in improving VVA symptoms. This study investigated the effects of fractional CO2 laser in post-menopausal women treated by resurfacing and coagulation of the vaginal canal tissues and mucosal tissues of the introitus.
METHODS
Study Design
This prospective study was conducted at our outpatient clinic. Study participants included 20 post-menopausal women presenting to the clinic with symptoms of VVA (vaginal dryness, irritation, soreness, or dyspareunia associated with this condition), stress or urge urinary incontinence. Patients with history of previous vaginal reconstructive surgery or treatment for vaginal tightening within the past 12 months, acute or recurrent urinary tract infections, active genital infections, hormonal imbalance or any serious conditions which could impair compliance were excluded from the study. Prior to treatment a vaginal examination was done to ensure eligibility and determine the vaginal health index score (VHIS) performed at all visits.
Study Protocol
All eligible patients received fractional CO2 treatments (Lumenis FemTouch TM) intravaginally using the specific vaginal hand piece. Treatment of the vaginal canal was performed using the square pattern and deep mode with the internal handpiece, fractional density of 5-15% and energy level of 7.5-12.5 mJ. The speculum cage was introduced into the introitus, and the handpiece was inserted to the interior edge of the treatment site (up to 11 cm in the vaginal canal). Several drops of baby oil were used for more comfortable insertion into the introitus. The handpiece was positioned with contact to the vaginal wall and pulses were applied at each 1 cm marking and then retracted, until a 4-5 cm depth. The handpiece was rotated 45°-90° to ensure all areas were treated uniformly (Figure 1).
Figure 1. The Procedure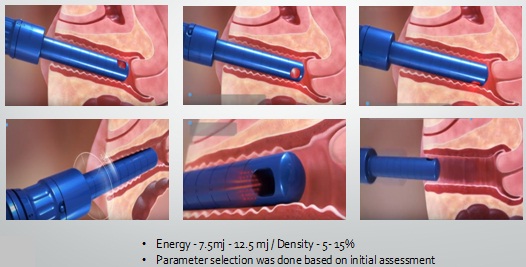
Subjects received three treatments at 1-month interval. The procedure was performed in the outpatient clinic and did not require analgesia/anesthesia. Patients were recommended to avoid coital sexual activity and tampon use for at least 7-days after treatment.
The objective of the study was to study the efficacy of CO2 laser in the improvement of vulvovaginal atrophy, stress urinary incontinence, urge incontinence, vaginal laxity and sexual functioning.
Data Assessment
Vaginal health index score (VHIS) was determined at all visits. Subjective evaluation of VVA symptoms were assessed using the visual analog scale (VAS) at all visits. Sexual functioning was evaluated using the female sexual function index (FSFI) questionnaire. Urinary Incontinence was evaluated using the Incontinence- QoL (I-QoL) questionnaire. Differences between baseline and follow-up VHI scores were analyzed with Wilcoxon signed-rank test for paired data. Statistical significance was set at p<0.05.
RESULTS
The study included 20 post-menopausal women (mean age 56±7 years) treated at three sessions with fractional CO2 laser. Patients were assessed following each treatment and at the 1-month follow-up after the final treatment.
Vaginal Health Index Score
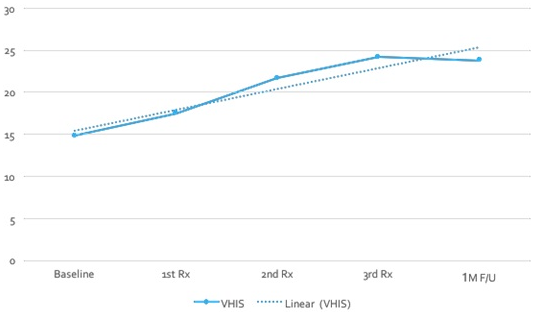
At baseline, the mean VHI score in the peri-menopausal study population was 15.1±1.6 (range 15-18). Vaginal health improved significantly with successive treatments with a mean improvement of 4.8 points in the VHI at 1-month follow-up post-third treatment. All the patients showed a statistically significant increase in the VHI score (p<0.05, Wilcoxon signed-rank test for paired data) with a mean score of 24.0±2.1 (range 22-26) (Figure 2).
Figure 2. Vaginal Health Index Score
Visual Analog Scale Scoring of Visual Analog Scale Symptoms
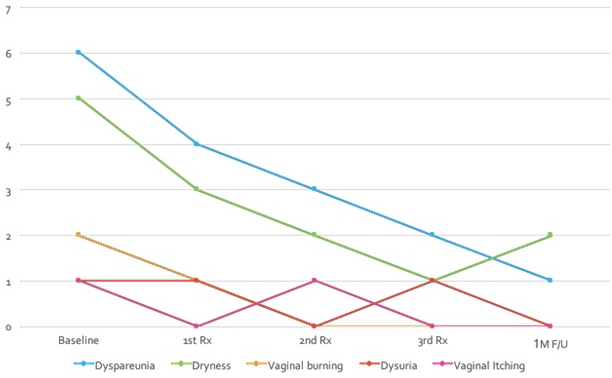
There was improvement noted in all symptoms when compared to baseline with symptoms like dyspareunia, dryness and vaginal burning showing significant improvement. Ninety-four percent of patients showed remarkable improvement in dyspareunia after the third session of treatment and continued to improve even on 1-month follow-up. Ninety-one percent showed significant improvement in vaginal dryness after the third session and 88% showed improvement in vaginal burning sensation. Other symptoms like dysuria and vaginal itching also seem to have improved (Figure 3).
Figure 3. VAS Scoring of VAS Symptoms
Female Sexual Function Index Sexual Functioning Questionnaire
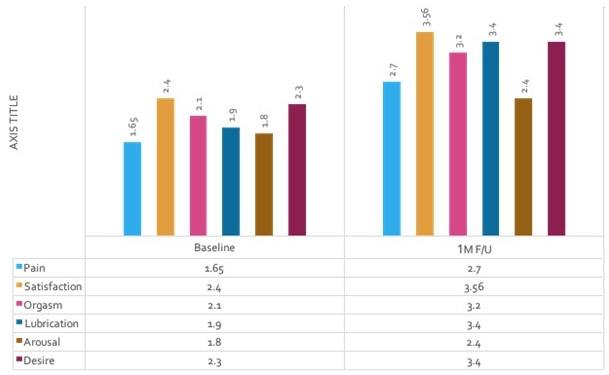
Subject assessment of vaginal and sexual functioning symptoms also improved with successive treatments. At 1-month following the third treatment, 90% of subjects reported an improvement in sexual gratification (more friction with a greater number and improved orgasms), and 94% reported an improvement in vaginal rejuvenation (increased vaginal tightening and improvement in dryness and atrophy). All subjects (100%) reported satisfaction with treatment and 94% would recommend the procedure (Figure 4).
Figure 4. FSFI Sexual Functioning Questionnaire
I-QOL scoring
I-QOL scoring was assessed using parameters like avoidance and limiting behavior, psychosocial impact and social embarassment. There were good improvement noted in all parameters with all 86% patients reporting some improvement post third treatment. All patients (100%) were interested in taking more treatments and were happy to return for future follow-ups as well.
Safety of Treatments
Treatments did not require analgesia/anesthesia. Mean treatment time, including examination of the area and prep (cleaning the treatment area with a disinfecting solution), was 21±3 minutes. Most patients (97%) reported that treatments were accompanied with no pain or minimal pain. Immediate treatment responses were mild and transient, resolving within 1-2 days and included burning sensation (25%), itching (10%), twinging sensation (5%) and numbness (3%). There were no treatment complications or adverse effects noted.
DISCUSSION
CO2 lasers have revolutionized dermatological and esthetic treatments by giving promising results consistently. With its property of tissue remodeling and regeneration through fractional ablation it has given a new foray into cosmetic treatments.
The CO2 energy is delivered in a fractional manner which generates controlled and precise tissue damage. It maintains healthy tissue surrounding each micro ablation zone enabling rapid and complete epithelial repair. Fractional scanner aids in deploying the exact amount of energy, rapidly and the depth of penetration is controllable to address the desired tissue and obtain optimal clinical effect. The energy delivered helps in effective tissue remodeling while ensuring safety of the fibromuscular layer by creating small controlled small ablation coagulation zones within the lamina propria using various energy levels.9
The heat generated with the CO2 laser induces a transient heat shock response and produces heat shock proteins (HSP). HSP 70 is over-expressed following laser ablation and plays a key role in the production of transforming growth factor-ß (TGF-ß). TGF-ß is a key element in the inflammatory response and the fibrogenic process. This in turn helps in collagenization and production of extracellular matrix.10
CO2 laser is capable of restoring the pH of the vaginal mucosa by liberating glycogen and acidic mucins from the epithelium. Symptoms of dryness and itching, dysuria, and recurrent infections can be alleviated by increasing the glycogen that rebalances lactobacilli, which inhibit the growth and virulence of pathogenic bacteria.11
Successive treatments may be required in these subjects for maintenance and long-term follow-ups will help us in understanding the long term effects of the treatments and the need for anymore sessions.
CONCLUSION
In our study, all the patients had significant improvement in most parameters analyzed. There was on overall improvement in vaginal health reported by all the patients. The sample size was relatively small considered to western studies where these treatments have gained popularity already. This may be attributed to the apprehensions that our patients have as the awareness about the positive outcomes from such treatments are yet to be realized. Larger cohorts may be required with long-term follow-up to completely understand the potential of such treatments. The challenge lies in the fact that there is still a huge number of patients who shy away from approaching clinicians with their concerns and their access to such treatments as only few centers in India have such lasers. Gynecologists can play a crucial role in appropriate referrals and help in familiarizing such treatment options.
CONFLICT OF INTERESTS
The authors declare that there is no conflict of interests regarding the publication of this paper.


