The National Institute on Drug Abuse (NIDA) defines longterm recovery as a process of change through which people improve their health and wellness, live self-directed lives, and strive to reach their full potential.1 Even people with severe and chronic substance use disorders can, with help, overcome their illness and regain health and social function; this is called remission.1
But as also poignantly stated by the NIDA Director, Dr. Nora Volkow, resolving the radiating impacts of a substance use disorder (SUD) on an individual’s life are also crucial elements of the recovery process.2 The Midwest is the latest region in the US to experience an epidemic of synthetic opioid substance abuse (fentanyl and analogues), following locales like Los Angeles, Miami, Pennsylvania, the Appalachian region, and practically the entire East Coast. Taken together, this epidemic is spreading across race, class, and region at a rate and extent that has NEVER been seen in the United States. This epidemic brings death and destruction in its wake.
This abuse epidemic brings to the fore one critical component of studies examining successful sustained recovery; it should include greater involvement of people with lived experience in research design, methodologies, and critical focal points of what elements aided their own experiences as they battled their own barriers to recovery. As stated by others, the science of “recovery supports” is emblematic of how successful that mindset can be. The Substance Abuse Subtle Screening Inventory (SASSI) Institute is providing this short commentary to hopefully provide a guiding template indicative of how the SUD field might discover these elements of “a successful recovery” experience from the perspective of those living their lives in remission. The SASSI Institute would like to provide the field with additional information documenting the successes and failures of various strategies utilized by substance use disordered individuals in long-term remission, and in their own words. Names and identifying information will not be given to protect anonymity and to comply with Health Insurance Portability and Accountability Act (HIPAA) guidelines. In order to capture the essence of an individual’s experience requires a first-person accounting of those successes and failures. Some of these conceptual elements include SUD and public health issues, hepatitis C (HCV), human immunodeficiency virus (HIV); self-perception – the “reality” that an individual ‘sees’ upon self-examination; reaction to labels and labeling; and as posited by Terry 2003, and later Tiburcio 2008, identity transformation.3-7
Recovery Movement
The long-term SUD treatment recovery movement as it has recently been referred to,8 dates back to the initial days of Synanon. Synanon stood as an acronym for “unknown togetherness”, that is, group anonymity.9 Proceeding in stages, Synanon became the forerunner to various other Therapeutic Communities, loosely based on the Synanon model. The basic tenets of all these modalities, however, were that in order to build an individual “up”, you must first “tear him/her down” so they could be fresh in their “new recovering personhood”. There were various stages and/or peer groups within the model. These included Assessment and Orientation (where the newly entering resident acclimated to the new environment). Orientation was followed by Main Treatment, where the real “recovery work” began. During this phase, residents engaged in various job functions, role-playing, confrontation, and counselor engagement. The earlier models of this treatment modality entailed the “Fear Concept” of addiction treatment (the “tear-down/build-up” model — see, for example, DeLeon 2000 and Tiburcio 2006).5,10 During the following decade/s, the Fear Concept morphed into the more resident-friendly “Sensitivity treatment model”. This model took sway during the era of “hugs-not-drugs”, harboring conceptual elements of treating substance-use-disordered individuals as sick, following the rubric of the disease model of addiction.4,7,11-15 Once the Main Treatment Phase was successfully completed, the individual was now deemed ready to “face the world” during the Re-Entry phase of treatment. Many, including those that had neither the necessary resources nor other recourse, found themselves housed in areas where the initiation of their substance use issues began. Prior research suggests that this may be the most difficult and onerous phase of the treatment experience.7 For the first time in many months, sometimes periods of a year or more, the individual is allowed back (sometimes forced back) into the community, despite having lived the previous months in a semi-protected state. The people, places, and things that led to their drug use and relapse experiences were now to be dealt with head-on. One former inpatient treatment resident, a participant in a previous Institutionally Reviewed Board (IRB) study, reflected on his experiences this way:
“it is very similar to be thrown into the deep end of the pool, but you have never swum before….”.7
Unfortunately, the original Synanon program and subsequent direct offshoots were eventually disbanded owing to various alleged transgressions, including being labeled a “cult”, as well as accusations of tax evasion, among other allegations. This led to incarceration as a resource, instead of treatment for a fascinating description of how this phenomenon came to be and some intuitive suggestions as to possible ways to address what has become even more dysfunctional in multiple ways.4 In any event, individuals who, for all other intents and purposes, should have been hospitalized (as in the case of a severe diabetic or late-stage cancer patient) were instead placed in the confines of a myriad maze of criminal justice institutions. Thus, any issues these individuals were already contending with were exacerbated, sometimes insurmountable. However, Synanon’s Therapeutic Community process for training recovering addicts with long criminal backgrounds and prison experience to become effective therapists for younger delinquents was a quintessential positive contribution of Synanon to society.16
But one thing is clear, labeling, stigmatization, and the negative feelings and attitudes these behaviors produce are undeniable. In addition to the emotional and psychological stigmatization these recovering individuals are exposed to, professional opportunities and pursuits are also curtailed, sometimes dramatically. In a public survey, attitudes were more negative towards people with addiction than towards those with mental illness, viewing addiction as a moral failing.17 The respondents, as shown in Figure 1, were more willing to accept discriminatory practices against persons with addiction, more skeptical about the effectiveness of treatments, and more likely to oppose policies aimed at helping them. These recovering individuals are now faced with a new reality, “a new normal”, as it were, where they are expected to resume a “normal” life immediately. Even though many were never given sufficient preparation and training to achieve their goals. These limitations to professional opportunities for these individuals enhance the risk of returning to non-conventional means of survival, particularly if faced with few other alternatives. Thus, the often-described cycle of recovery, relapse, treatment, detoxification, hospitalizations, increased exposures to arrests or incarceration, and renewed recovery attempts often resume after incarceration.6,7,18
Figure 1. Public Attitudes about Persons with Drug Addiction (N5347) and Mental Illness (N5362), 2013a
One of only a few studies that have conducted investigations comparing therapeutic community treatment modifications internationally and from the perspective of the participants themselves, while also considering cultural components of this process was completed in 2010.13 One key advantage of the resulting Qualitative datasets and analyses was that it not only contained residents’ perspectives, and staff experiential elements but importantly, incorporated staff debriefings about their respective interactions at each of the international treatment modalities, presenting well-rounded depictions of each of these milieus. The data demonstrated that the enhanced portrait of the provider-patient treatment dynamic was quite similar despite the changes in cultural milieus. This finding indeed lent voice to the various aspects of treatment participation while accounting for these cultural issues and from the perspective of providers, as well as the participants.
Considering the respondents’ voices and the impact of “peer support” on the recovery process necessarily includes achieving a clearer definition of what constitutes recovery for each of the respondents. Some have discussed the quality of their recovery.13 Others have defined recovery as the number of days, weeks, and months (years) of abstinence. The difficulty expressed by many of these individuals is that they found themselves “white-knuckling it” (going it alone) throughout their treatment experience, and later when back in the community, they inevitably failed. John, a longtime therapeutic community participant, explained it this way:
“Altogether, I would say I was in treatment for about four years if you count all the experiences…. but I didn’t learn anything. I didn’t pick up that I had to really buy into the program so that I could get better; it just never worked for me…” (Note: Unfortunately, John died of an overdose in 2019, four days after being released from yet another treatment episode).
Still, other treatment participants merge these concepts, describing their experience as a continuous period of extended sobriety.7 So, the question remains, is it quality, quantity, or a combination of both, or is there another approach that is clearly missing? Currently, the definition of treatment success reflects the values and practices of the people that are defining it.19 For example, in the criminal justice system, recovery usually must include that the offender-addict no longer commits crimes as this lack of recidivism is a goal. The SUD field must continue to strive for a much clearer understanding of what all these concepts entail. Otherwise, we find ourselves in various quagmires of what “success” (a label in and of itself!) looks and feels like or what constitutes its successful elements.
In 2001, a pilot research study was conducted to determine if rational recovery (RR), a self-empowering approach to SUD treatment that utilizes an individual’s cognitive ability to actively refuse certain destructive behaviors while choosing more healthy ones, enhanced the recovery process for early-stage addiction.20 This study utilized the SASSI as a measurement of symptoms associated with alcohol/drug use.21 This experimental research was designed to assess the efficacy of RR as a viable treatment alternative. The results of this study indicated that RR may be an effective alternative in promoting openness, thereby enhancing awareness and lessening denial. However, it is important to note that the SASSI screening tool is not validated or recommended to be used as a measure of treatment effectiveness. Future investigations utilizing the SASSI, or hybrids of the SASSI, when used as a pre and post-test measure are needed. The research team at the SASSI Institute is currently in the planning stages of developing such an instrument.
In 2005, the Center for Substance Abuse Treatment (CSAT), within the Substance Abuse and Mental Health Services Administration (SAMHSA) held the first National Summit on Recovery to enable a diverse group of participants to interact and engage in dialogue about recovery.22 Definitions and principles developed at the summit are continually evolving. The most recent definition is from 2011: “Recovery is a process of change whereby individuals improve their health and wellness, to live a self-directed life, and strive to reach their full potential”.23 The SASSI Institute agrees with this concept and previously provided a similar definition of recovery: “Recovery is a process of courageously seeking to make changes necessary to enjoy a rich and satisfying life”.24 The SASSI Institute provides screening tools to help individuals gain the necessary awareness to transform their lives and thereby restore health and well-being. Some of these include the SASSI for adults, adolescents, and Spanish-speaking adults.25,26,27
Nearly thirty years ago, Sampson and Laub 1993, argued that by achieving social capital, adults are able to strengthen social bonds, which in combination with turning points in the life course, play a pivotal role in understanding change processes.28 Although for recovering individuals, it cannot be conclusively stated that any one of these events will be instrumental to their abstinence efforts, collectively, it appears that the combination of events will indeed strengthen their change processes. Establishing stakes in conformity will enable their recovery efforts and deter them from engaging in past deleterious behaviors. But the key for those that will do it successfully is the opportunity to do so. Historically, these individuals have referred to their having had the opportunity to change their lives. It was not simply the desire to do so, although, of course, that played a pivotal role as well, but the opportunity to turn their lives around was instrumental to their maintained lifestyle changes. It is certainly understandable why some might have no recourse other than to resort to public assistance and other such programs; if they are refused employment in practically all places, they seek it. But secondly, if when factoring in the costs of going to a minimum wage job, the resulting wage is less than what they received by engaging in some government program, it practically serves as a disincentive to work. Despite this, many did work. As shown elsewhere, some even admitted to being embarrassed at the type of work they had to do initially, but they forged ahead in search of a better, sober life.5
The SASSI Institute remains interested in examining those that have experienced the vast dangers of analogue drugs (Fentanyl, Carfentanil, etc.), yet have survived. Many of these individuals were emotionally and psychically dead, if not physically. These experiences should be examined. The SUD field needs to achieve a greater understanding of the pipelines bringing these dangerous drugs past our borders and carefully examine the many barriers that confront us in the future. The SASSI Institute has already begun this process. An important first step is a close alignment with various local peer-to-peer support networks. These individuals on the treatment pipeline’s front lines will help sustain important community-based participatory research footprints. Fostering and developing multiple communities of support services, initially on a local level, but then expanding these collaborations throughout the Midwestern United States and then throughout the country will enable a stronger understanding of the barriers present in achieving long-term success. Subsequently, international collaborations of these types will further this understanding.
CONCLUSION
Exploring and supporting therapies based on nuanced “learning model/s” of substance abuse and addiction, as well as more traditional models, will provide enhancements to the recovery treatment field and foster a better understanding of the participants themselves. Clearly, the SUD treatment community has reached a point where a common dictum that has been passed around for years within Harm Reduction Communities should now become a mandate: “Nothing about us, without us!” This phrase stems from a document originally researched and reported by Jürgens.29 The intent was and is to promote public health approaches to dealing with problems of illegal drug use. To do this requires acknowledging that drug supply-control strategies are limited in their effectiveness and can sometimes be counter-productive and that approaches to drug treatment based on abstinence are also limited. The recovery process is highly personal and occurs via many pathways. The various treatment models that have shown success may include medication-assisted treatment, clinical treatment, faith-based approaches, family support, peer-based support services, self-care, hospital inpatient, short-term inpatient rehabilitation, long-term residential, outpatient, and twelve-step meeting participation, among other approaches.
It is time to examine the experiences, strengths, hopes, and barriers of those who have succeeded in achieving long-term sobriety from substance use disorder, so these can inform and assist others.
CONFLICTS OF INTEREST
The authors declare that they have no conflicts of interest.
Social Behavior Research and Practice
Open journal
ISSN 2474-8927
Examining Sustained Recovery from Substance Use Disorder — A Delicate Process
Nelson J. Tiburcio* and Scarlett L. Baker
Nelson J. Tiburcio, PhD
CEO, The SASSI Institute, Springville, IN 47462, USA; Phone. 800-726-0526; Fax. 800-546-7995; E-mail: research@sassi.com
The National Institute on Drug Abuse (NIDA) defines longterm recovery as a process of change through which people improve their health and wellness, live self-directed lives, and strive to reach their full potential.1 Even people with severe and chronic substance use disorders can, with help, overcome their illness and regain health and social function; this is called remission.1
But as also poignantly stated by the NIDA Director, Dr. Nora Volkow, resolving the radiating impacts of a substance use disorder (SUD) on an individual’s life are also crucial elements of the recovery process.2 The Midwest is the latest region in the US to experience an epidemic of synthetic opioid substance abuse (fentanyl and analogues), following locales like Los Angeles, Miami, Pennsylvania, the Appalachian region, and practically the entire East Coast. Taken together, this epidemic is spreading across race, class, and region at a rate and extent that has NEVER been seen in the United States. This epidemic brings death and destruction in its wake.
This abuse epidemic brings to the fore one critical component of studies examining successful sustained recovery; it should include greater involvement of people with lived experience in research design, methodologies, and critical focal points of what elements aided their own experiences as they battled their own barriers to recovery. As stated by others, the science of “recovery supports” is emblematic of how successful that mindset can be. The Substance Abuse Subtle Screening Inventory (SASSI) Institute is providing this short commentary to hopefully provide a guiding template indicative of how the SUD field might discover these elements of “a successful recovery” experience from the perspective of those living their lives in remission. The SASSI Institute would like to provide the field with additional information documenting the successes and failures of various strategies utilized by substance use disordered individuals in long-term remission, and in their own words. Names and identifying information will not be given to protect anonymity and to comply with Health Insurance Portability and Accountability Act (HIPAA) guidelines. In order to capture the essence of an individual’s experience requires a first-person accounting of those successes and failures. Some of these conceptual elements include SUD and public health issues, hepatitis C (HCV), human immunodeficiency virus (HIV); self-perception – the “reality” that an individual ‘sees’ upon self-examination; reaction to labels and labeling; and as posited by Terry 2003, and later Tiburcio 2008, identity transformation.3-7
Recovery Movement
The long-term SUD treatment recovery movement as it has recently been referred to,8 dates back to the initial days of Synanon. Synanon stood as an acronym for “unknown togetherness”, that is, group anonymity.9 Proceeding in stages, Synanon became the forerunner to various other Therapeutic Communities, loosely based on the Synanon model. The basic tenets of all these modalities, however, were that in order to build an individual “up”, you must first “tear him/her down” so they could be fresh in their “new recovering personhood”. There were various stages and/or peer groups within the model. These included Assessment and Orientation (where the newly entering resident acclimated to the new environment). Orientation was followed by Main Treatment, where the real “recovery work” began. During this phase, residents engaged in various job functions, role-playing, confrontation, and counselor engagement. The earlier models of this treatment modality entailed the “Fear Concept” of addiction treatment (the “tear-down/build-up” model — see, for example, DeLeon 2000 and Tiburcio 2006).5,10 During the following decade/s, the Fear Concept morphed into the more resident-friendly “Sensitivity treatment model”. This model took sway during the era of “hugs-not-drugs”, harboring conceptual elements of treating substance-use-disordered individuals as sick, following the rubric of the disease model of addiction.4,7,11-15 Once the Main Treatment Phase was successfully completed, the individual was now deemed ready to “face the world” during the Re-Entry phase of treatment. Many, including those that had neither the necessary resources nor other recourse, found themselves housed in areas where the initiation of their substance use issues began. Prior research suggests that this may be the most difficult and onerous phase of the treatment experience.7 For the first time in many months, sometimes periods of a year or more, the individual is allowed back (sometimes forced back) into the community, despite having lived the previous months in a semi-protected state. The people, places, and things that led to their drug use and relapse experiences were now to be dealt with head-on. One former inpatient treatment resident, a participant in a previous Institutionally Reviewed Board (IRB) study, reflected on his experiences this way:
“it is very similar to be thrown into the deep end of the pool, but you have never swum before….”.7
Unfortunately, the original Synanon program and subsequent direct offshoots were eventually disbanded owing to various alleged transgressions, including being labeled a “cult”, as well as accusations of tax evasion, among other allegations. This led to incarceration as a resource, instead of treatment for a fascinating description of how this phenomenon came to be and some intuitive suggestions as to possible ways to address what has become even more dysfunctional in multiple ways.4 In any event, individuals who, for all other intents and purposes, should have been hospitalized (as in the case of a severe diabetic or late-stage cancer patient) were instead placed in the confines of a myriad maze of criminal justice institutions. Thus, any issues these individuals were already contending with were exacerbated, sometimes insurmountable. However, Synanon’s Therapeutic Community process for training recovering addicts with long criminal backgrounds and prison experience to become effective therapists for younger delinquents was a quintessential positive contribution of Synanon to society.16
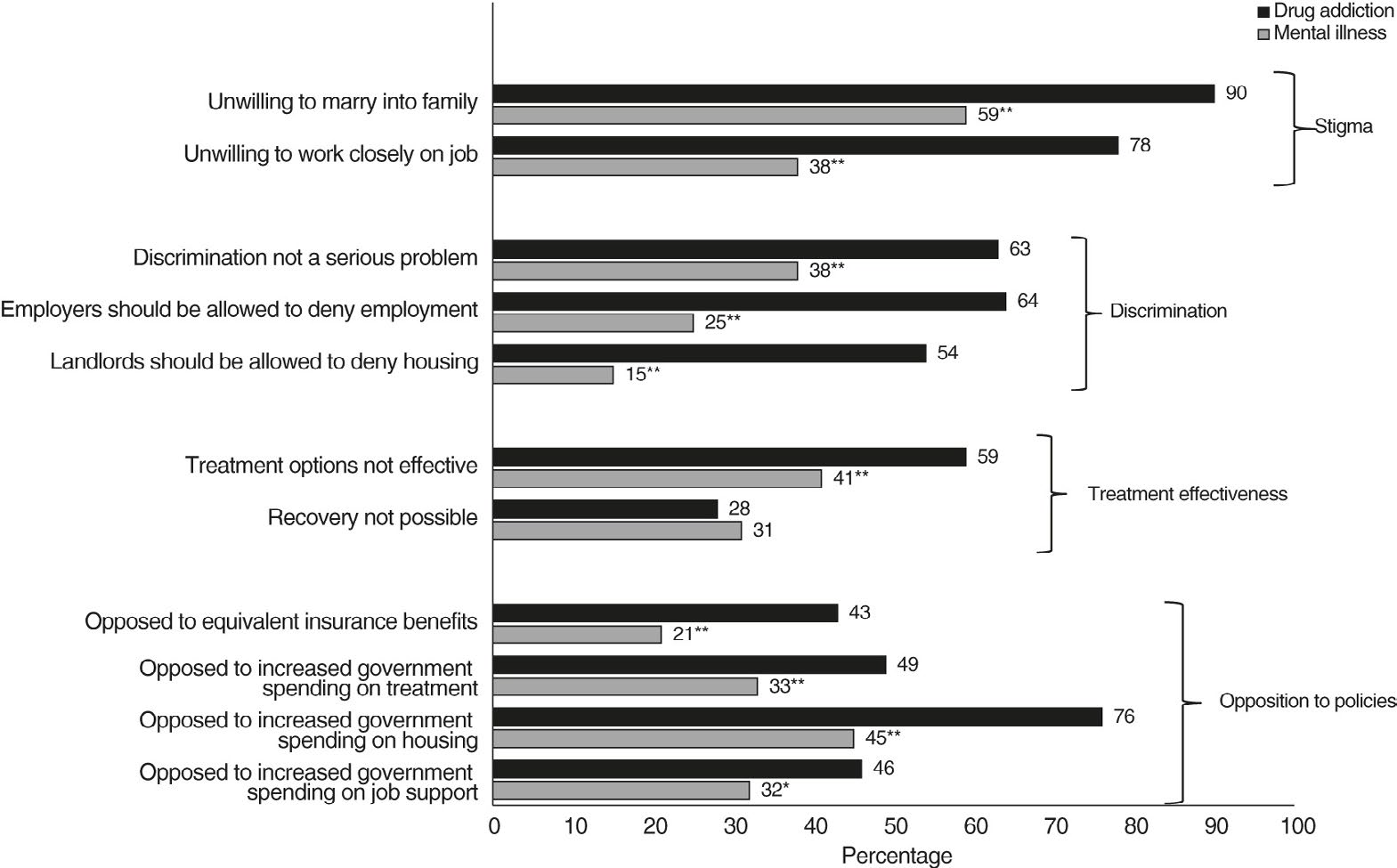
But one thing is clear, labeling, stigmatization, and the negative feelings and attitudes these behaviors produce are undeniable. In addition to the emotional and psychological stigmatization these recovering individuals are exposed to, professional opportunities and pursuits are also curtailed, sometimes dramatically. In a public survey, attitudes were more negative towards people with addiction than towards those with mental illness, viewing addiction as a moral failing.17 The respondents, as shown in Figure 1, were more willing to accept discriminatory practices against persons with addiction, more skeptical about the effectiveness of treatments, and more likely to oppose policies aimed at helping them. These recovering individuals are now faced with a new reality, “a new normal”, as it were, where they are expected to resume a “normal” life immediately. Even though many were never given sufficient preparation and training to achieve their goals. These limitations to professional opportunities for these individuals enhance the risk of returning to non-conventional means of survival, particularly if faced with few other alternatives. Thus, the often-described cycle of recovery, relapse, treatment, detoxification, hospitalizations, increased exposures to arrests or incarceration, and renewed recovery attempts often resume after incarceration.6,7,18
Figure 1. Public Attitudes about Persons with Drug Addiction (N5347) and Mental Illness (N5362), 2013a
One of only a few studies that have conducted investigations comparing therapeutic community treatment modifications internationally and from the perspective of the participants themselves, while also considering cultural components of this process was completed in 2010.13 One key advantage of the resulting Qualitative datasets and analyses was that it not only contained residents’ perspectives, and staff experiential elements but importantly, incorporated staff debriefings about their respective interactions at each of the international treatment modalities, presenting well-rounded depictions of each of these milieus. The data demonstrated that the enhanced portrait of the provider-patient treatment dynamic was quite similar despite the changes in cultural milieus. This finding indeed lent voice to the various aspects of treatment participation while accounting for these cultural issues and from the perspective of providers, as well as the participants.
Considering the respondents’ voices and the impact of “peer support” on the recovery process necessarily includes achieving a clearer definition of what constitutes recovery for each of the respondents. Some have discussed the quality of their recovery.13 Others have defined recovery as the number of days, weeks, and months (years) of abstinence. The difficulty expressed by many of these individuals is that they found themselves “white-knuckling it” (going it alone) throughout their treatment experience, and later when back in the community, they inevitably failed. John, a longtime therapeutic community participant, explained it this way:
“Altogether, I would say I was in treatment for about four years if you count all the experiences…. but I didn’t learn anything. I didn’t pick up that I had to really buy into the program so that I could get better; it just never worked for me…” (Note: Unfortunately, John died of an overdose in 2019, four days after being released from yet another treatment episode).
Still, other treatment participants merge these concepts, describing their experience as a continuous period of extended sobriety.7 So, the question remains, is it quality, quantity, or a combination of both, or is there another approach that is clearly missing? Currently, the definition of treatment success reflects the values and practices of the people that are defining it.19 For example, in the criminal justice system, recovery usually must include that the offender-addict no longer commits crimes as this lack of recidivism is a goal. The SUD field must continue to strive for a much clearer understanding of what all these concepts entail. Otherwise, we find ourselves in various quagmires of what “success” (a label in and of itself!) looks and feels like or what constitutes its successful elements.
In 2001, a pilot research study was conducted to determine if rational recovery (RR), a self-empowering approach to SUD treatment that utilizes an individual’s cognitive ability to actively refuse certain destructive behaviors while choosing more healthy ones, enhanced the recovery process for early-stage addiction.20 This study utilized the SASSI as a measurement of symptoms associated with alcohol/drug use.21 This experimental research was designed to assess the efficacy of RR as a viable treatment alternative. The results of this study indicated that RR may be an effective alternative in promoting openness, thereby enhancing awareness and lessening denial. However, it is important to note that the SASSI screening tool is not validated or recommended to be used as a measure of treatment effectiveness. Future investigations utilizing the SASSI, or hybrids of the SASSI, when used as a pre and post-test measure are needed. The research team at the SASSI Institute is currently in the planning stages of developing such an instrument.
In 2005, the Center for Substance Abuse Treatment (CSAT), within the Substance Abuse and Mental Health Services Administration (SAMHSA) held the first National Summit on Recovery to enable a diverse group of participants to interact and engage in dialogue about recovery.22 Definitions and principles developed at the summit are continually evolving. The most recent definition is from 2011: “Recovery is a process of change whereby individuals improve their health and wellness, to live a self-directed life, and strive to reach their full potential”.23 The SASSI Institute agrees with this concept and previously provided a similar definition of recovery: “Recovery is a process of courageously seeking to make changes necessary to enjoy a rich and satisfying life”.24 The SASSI Institute provides screening tools to help individuals gain the necessary awareness to transform their lives and thereby restore health and well-being. Some of these include the SASSI for adults, adolescents, and Spanish-speaking adults.25,26,27
Nearly thirty years ago, Sampson and Laub 1993, argued that by achieving social capital, adults are able to strengthen social bonds, which in combination with turning points in the life course, play a pivotal role in understanding change processes.28 Although for recovering individuals, it cannot be conclusively stated that any one of these events will be instrumental to their abstinence efforts, collectively, it appears that the combination of events will indeed strengthen their change processes. Establishing stakes in conformity will enable their recovery efforts and deter them from engaging in past deleterious behaviors. But the key for those that will do it successfully is the opportunity to do so. Historically, these individuals have referred to their having had the opportunity to change their lives. It was not simply the desire to do so, although, of course, that played a pivotal role as well, but the opportunity to turn their lives around was instrumental to their maintained lifestyle changes. It is certainly understandable why some might have no recourse other than to resort to public assistance and other such programs; if they are refused employment in practically all places, they seek it. But secondly, if when factoring in the costs of going to a minimum wage job, the resulting wage is less than what they received by engaging in some government program, it practically serves as a disincentive to work. Despite this, many did work. As shown elsewhere, some even admitted to being embarrassed at the type of work they had to do initially, but they forged ahead in search of a better, sober life.5
The SASSI Institute remains interested in examining those that have experienced the vast dangers of analogue drugs (Fentanyl, Carfentanil, etc.), yet have survived. Many of these individuals were emotionally and psychically dead, if not physically. These experiences should be examined. The SUD field needs to achieve a greater understanding of the pipelines bringing these dangerous drugs past our borders and carefully examine the many barriers that confront us in the future. The SASSI Institute has already begun this process. An important first step is a close alignment with various local peer-to-peer support networks. These individuals on the treatment pipeline’s front lines will help sustain important community-based participatory research footprints. Fostering and developing multiple communities of support services, initially on a local level, but then expanding these collaborations throughout the Midwestern United States and then throughout the country will enable a stronger understanding of the barriers present in achieving long-term success. Subsequently, international collaborations of these types will further this understanding.
CONCLUSION
Exploring and supporting therapies based on nuanced “learning model/s” of substance abuse and addiction, as well as more traditional models, will provide enhancements to the recovery treatment field and foster a better understanding of the participants themselves. Clearly, the SUD treatment community has reached a point where a common dictum that has been passed around for years within Harm Reduction Communities should now become a mandate: “Nothing about us, without us!” This phrase stems from a document originally researched and reported by Jürgens.29 The intent was and is to promote public health approaches to dealing with problems of illegal drug use. To do this requires acknowledging that drug supply-control strategies are limited in their effectiveness and can sometimes be counter-productive and that approaches to drug treatment based on abstinence are also limited. The recovery process is highly personal and occurs via many pathways. The various treatment models that have shown success may include medication-assisted treatment, clinical treatment, faith-based approaches, family support, peer-based support services, self-care, hospital inpatient, short-term inpatient rehabilitation, long-term residential, outpatient, and twelve-step meeting participation, among other approaches.
It is time to examine the experiences, strengths, hopes, and barriers of those who have succeeded in achieving long-term sobriety from substance use disorder, so these can inform and assist others.
CONFLICTS OF INTEREST
The authors declare that they have no conflicts of interest.
1. National Institute on Drug Abuse (NIDA). Research Topics/ Recovery/About Recovery. 2022. Website. https://nida.nih.gov/ research-topics/recovery. Accessed November 11, 2022.
2.Volkow N. Nora’s Blog: Supporting Needed Research in Recovery. 2022. Website. https://nida.nih.gov/about-nida/noras-blog/2022/09/supporting-needed-research-recovery. Accessed November 11, 2022.
3. Strauss SM, Munoz-Plaza C, Tiburcio NJ, et al. Barriers and facilitators to undergoing hepatitis C virus (HCV) testing through drug treatment programs. Journal of Drug Issues. 2008; 38(4): 1161- 1185. doi: 10.1177/002204260803800411
4. Hampton R. Inside the Opioid Addiction Crisis – And how to end it: American Fix. New York, NY, USA: All Points Books; 2020.
5. Tiburcio NJ. Five Years After: The Process of Long-term Abstinence from Heroin Use Among Ex-offenders [Microfilm]. New York, NY, USA: City University of New York Graduate Center; 2006.
6. Terry C. The Fellas: Overcoming Prison and Addiction. Belmont, CA, USA: Wadsworth; 2003.
7. Tiburcio NJ. Long-term recovery from heroin use among female ex-offenders: Marisol’s story. Subst Use Misuse. 2008; 43(12- 13): 1950-1970. doi: 10.1080/10826080802297369
8. Indiana Annual Recovery Month Symposium. Join us for the 14th Indiana Annual Recovery Month Symposium. 2022. Website. https://www.overdoselifeline.org/events/in-arms-symposium/. Accessed September 26, 2022.
9. Ofshe R. The social development of the synanon cult. Sociological Analysis. 1980; 41(2): 109-127. doi: 10.2307/3709903
10. DeLeon G. The Therapeutic Community Theory, Model and Method. New York, NY, USA: Springer Publishing; 2000.
11. Wixon L, Krauss J. Playing the Game: The Origins and Impact of Synanon. 2022. Website. https://www.breakingcodesilence. org/playing-the-game/. Accessed November 26, 2022.
12. Volkow N, Li TK. The neuroscience of addiction. Nat Neurosci. 2005; 8, 1429-1430. doi: 10.1038/nn1105-1429
13. Tiburcio NJ, Kressel D. An enhanced understanding of therapeutic communities worldwide. Rev Adiccion Cienc. 2011; 1(4).
14. National Institute on Drug Abuse (NIDA). Principles of Drug Addiction Treatment: A Research-Based Guide (Third Edition). 2014. Website. https://nida.nih.gov/sites/default/files/podat-3rdEd-508.pdf 11/29/22. Accessed November 26, 2022.
15. US Department of Health and Human Services (HHS), Office of the Surgeon General. Facing Addiction in America: The Surgeon General’s Report on Alcohol, Drugs, and Health. 2016. Website. https://pubmed.ncbi.nlm.nih.gov/28252892/. Accessed November 29, 2022.
16. Yablonsky L. Whatever happened to synanon? The Birth of the Anticriminal Therapeutic Community Methodology. Criminal Justice Policy Review. 2002; 13(4): 329-336. doi: 10.1177/088740302237802
17. Barry C, McGinty EE, Pescosolido, B, Goldman, HH. Stigma, discrimination, treatment effectiveness and policy support: Comparing public views about drug addiction with mental illness. Psychiatr Serv. 2014; 65(10), 1269-1272. doi: 10.1176/appi.ps.201400140
18. Maruna S. Making Good: How Ex-convicts Reform and ReBuild their Lives. Washington, DC, USA: American Psychological Association Books; 2001.
19. Osborne Jr, DR. You Can’t Fall Out of a Hole: Ripping the Band Aid Off of Our Addiction Epidemic. Meadville, PA, USA: Fulton Books; 2021.
20. Schmidt EA, Carns A, Chandler C. Assessing the efficacy of rational recovery in the treatment of alcohol/drug dependency. Alcoholism Treatment Quarterly. 2001; 19(1): 97-106. doi: 10.1300/J020v19n01_07
21. Miller GA. The Substance Abuse Subtle Screening Inventory (SASSI): Adult SASSI-2 manual supplement. Spencer, IN, USA: Spencer Evening World; 1994.
22. Center for Substance Abuse Treatment (CSAT). National Summit on Recovery Conference Report. 2005. Website. https:// www.opioidlibrary.org/wpcontent/uploads/2019/07/SAMHSA_WorkingDefRecovery_2005.pdf. Accessed December 7, 2022.
23. Substance Abuse and Mental Health Service’s Administration (SAMHSA). SAMHSA’s Working Definition of Recovery. 2012. Website. https://store.samhsa.gov/sites/default/files/d7/priv/ pep12-recdef.pdf. Accessed December 7, 2022.
24. Miller FG, Lazowski LE. The Substance Abuse Subtle Screening Inventory-3 (SASSI-3) Manual. Springville, IN, USA: The SASSI Institute; 1999.
25. Lazowski LE, Geary BB. Validation of the adult Substance Abuse Subtle Screening Inventory-4 (SASSI-4). European Journal of Psychological Assessment. 2019; 35(1): 86-97. doi: 10.1027/1015- 5759/a000359
26. Tiburcio NJ, Hanauer M, Baker SL. Validation of the Adolescent Substance Abuse Subtle Screening Inventory-3 (SASSI-A3). J Addict Res Ther. 2020; 11(5): 400. doi: 10.4172/2155-6105.1000400
27. Lazowski LE, Boye MW, Miller GA, Miller FG. The Development and Validation of the Spanish SASSI. Springville, IN, USA: The SASSI Institute; 2002.
28. Sampson R, Laub J. Crime in the Making: Pathways and Turning Points Through Life. London, UK: Harvard University Press; 1993.doi:10.2307/3340743
29. Jürgens R. “Nothing about us without us” — Greater, meaningful involvement of people who use illegal drugs: A public health, ethical, and human rights imperative. 2008. http://www. hivlegalnetwork.ca/site/wpcontent/uploads/2013/04/Greater+Involvement+-+Bklt+-+Drug+Policy+-+ENG.pdf. Accessed November 29, 2022.
LATEST ARTICLES
Study on Major Health and Constraints of Backyard and Commercial Poultry Production in Hawassa and Yirgalem Town, Southern Ethiopia
Amanuel P. Beta, Dereje Abera, Legese Belayneh and Isayas A. Kebede
doi.
Unraveling the Mysteries of Type-A Aortic Dissection Using POCUS/Echocardiography
Syeda Rukh*, Sathyanarayana Machani and Milind Awale
doi.
Do they Play or Flirt? ‘Pawsitive’ Correlations of Castration Status and Social Behaviour of Male Dogs (Canis lupus familiaris): Video Analyses and Questionnaires
Carina A. Kolkmeyer* and Udo Gansloßer
doi.
Assessment of Hygienic Practice, Isolation and Antimicrobial Susceptibility Test of E. coli from Honey Bees Farms in and Around Haramaya University and Haramaya Woreda, Ethiopia
Ahmedyasin M. Aliyi*, Adem Hiko, Abdallahi Abdureman and Mohammedkemal M. Ame
doi.
Employee Retention Model for the IT/ITES Sector: Embed your Employees through C.A.R.E and Retain them
Tanvi Chaturvedi*
doi.
Hypertriglyceridemia-Induced Pancreatitis: A Case Report and Literature Review
Maarten Bulterys, Melvin Willems* and Agnes Meersman
doi.
From Neck Pain to a Life-Threatening Condition: A Case Report
Floris Vandewoude* and Sören Verstraete
doi.
Facial Rejuvenation and Patients Satisfaction with the Fourth Generation of Aptos P(LA/CL)–Hyaluronic Acid Threads: A 12-Month Study
Albina Kajaia*
doi.
Effective Management of Refractory Folliculitis Decalvans Using Secukinumab
Adel Al-Santali and Wasan Al-Qurashi*
doi.
LATEST ARTICLES
Cross Sectional Study
2024 Jul
Study on Major Health and Constraints of Backyard and Commercial Poultry Production in Hawassa and Yirgalem Town, Southern Ethiopia
Case Report
2024 Jul
Unraveling the Mysteries of Type-A Aortic Dissection Using POCUS/Echocardiography
Original Research
2024 Jul
Do they Play or Flirt? ‘Pawsitive’ Correlations of Castration Status and Social Behaviour of Male Dogs (Canis lupus familiaris): Video Analyses and Questionnaires