INTRODUCTION
Post-traumatic stress disorder (PTSD) is a prevalent and potentially debilitating condition that typically occurs as a result of exposure to physical violence, natural disasters, emotional distress, or other severe stressors. This condition is continuously becoming more prominent globally.1,2 Australia in particular is facing a potential mental health crisis, with PTSD being a large contributor. Numerous studies have called attention to high rates of PTSD across various cohorts in Australia. In a 2020 nationwide survey, 25.60% (727/2840) of respondents reported symptoms that fulfilled the criteria of PTSD diagnosis, with a disproportionately large effect on women and younger individuals.3 Notable stressors include the coronavirus disease-2019 (COVID-19) pandemic, and climate change-related stressors, such as summer wildfires, amongst others. Specifically, ecological disasters took a toll on the Australian population. Emergency services personnel and Australian Defense Force personnel were more severely impacted, with PTSD prevalence rates being as high as 10% and 8.3% respectively, vs. the general population rate of 4.4% as reported by Dr Wallace in 2020.4 Rescue workers in particular have been shown to have a PTSD prevalence much greater than the general population, with rates reaching up to 46%.5 This current report aims to focus on a possible solution for PTSD in the Australian cohort by utilizing cervical sympathetic blockade (CSB).
Current PTSD Treatment Options
Many treatment guidelines and modalities are in place for PTSD globally, with forms of psychotherapy and pharmaceuticals being first-line. In the United States of America (USA), the Department of Veterans Affairs and Department of Defense Clinical Practice Guidelines for PTSD (2017) lists a variety of treatment options, with prolonged exposure (PE) therapy, cognitive processing therapy (CPT) and eye movement desensitization and reprocessing (EMDR) still having the strongest evidence base, particularly in military personnel and veterans. Accordingly, The US Department of Veterans Affairs has mandated that all veterans treated for PTSD have access to either prolonged exposure therapy or cognitive processing therapy.6 However, US veterans remain reluctant to seek care, with half of those in need not utilizing mental health services. Among veterans who begin PTSD treatment with psychotherapy or medication, drop-out rates are reported to be as high as 20-40% in randomized clinical trials and considerably higher in routine practice.7 While therapeutic efficacy is reported to be achieved in 60-80% of patients compliant with medical treatment, approximately 40% of patients drop out due to the prolonged time required for an effect, accounting for patients not completing treatment.7
In Australia, similar issues persist, where only one in five Australian Emergency Service first responders with probable PTSD (per DSM-5 criteria) received adequate help. It’s reasonable to consider the perception of treatment to be a factor, as 20% of those with probable PTSD who felt they needed support either did not seek or receive help.8
Cervical Sympathetic Block for PTSD Background
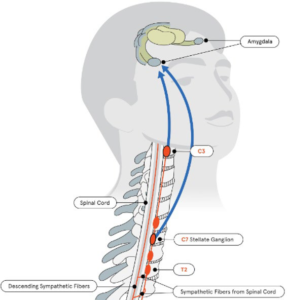
Recent research has shown that stellate ganglion block (SGB) is a viable therapy for the alleviation of PTSD symptoms. In this procedure, a local anesthetic is injected near the cervical sympathetic ganglion, usually at the level of the 6th cervical vertebra (C6). This inhibits sympathetic activity to the brain as well as the upper extremity and face. The first report of sympathetic modulation to treat PTSD was authored by Telaranta et al9 who performed endoscopic thoracic sympathetic clipping at the T-2 level for hand sweats and noted the resolution of PTSD symptoms in 1998. Dr. Telerate’s finding prompted Dr. Lipov to treat a survivor of a violent crime with Stellate Ganglion Block and report his findings in 2008.10 This was due to the anatomic fact that the highest sympathetic fiber leaving the spinal cord is at the T-2 level, which then ascends to the Stellate Ganglion, and finally to the brain (Figure 1).11
Figure 1. Base State/No Truma State
Since 2008, several studies have shown the efficacy of SGB for PTSD. Most notable of which was a 2019 randomized clinical study (RCT) consisting of 113 patients, in which the treatment group demonstrated significantly improved scores on assessments of PTSD-associated symptoms, distress, anxiety, pain symptoms, physical functioning, and mental functioning compared to placebo. The active treatment group had a response rate twice that of the placebo group.12 Multiple case reports have documented SGB efficacy for treating PTSD. Furthermore, the cervical sympathetic block has been advanced to blockade C6 and C4 levels (where superior cervical ganglion (SCG) is targeted) and is currently performed due to improved efficacy.13 Thus, the term used in this paper is CSB, which denotes C6 and C3/C4 sympathetic blockade.
METHODS
The patient was given information concerning the risks/benefits of the procedure and a consent form was completed. The inclusion criteria were patients having PTSD diagnosis. Exclusion criteria were an unstable mental state, active psychosis, being physically stable for CSB, or being anticoagulated. An intravenous line was started with a 22G IV in the left hand. Following sedation or local anesthetic as per patient preference, the patient was placed in a supine position, and appropriate ASA-mandated monitors were placed. The patient was positioned comfortably in the supine position and prepped and draped in a sterile fashion. The skin over the anterior and right side of the neck was cleaned with chlorhexidineisopropyl alcohol preparation. Fluoroscopy (GE 1999) was used to identify the C-6 vertebral level transverse process. The skin at the injection site on the lateral neck was anesthetized with 1 mL of 1% lidocaine. A 22-gauge, 3.5-inch Quincke needle was inserted to the appropriate depth where contact was made with the ventrolateral aspect of the C6 vertebral body. The needle was withdrawn at 1 mm. Lateral view of the spine was obtained and the needle tip was confirmed to be dorsal to the ventral aspect of the vertebral body. After a negative attempted aspiration, while monitoring the patient, 1.0 mL of Isovue-200 was injected under fluoroscopic guidance. If intravascular spread was identified or spread was not noted along the cephalad and caudal aspect longus colli muscle belly, the needle tip was repositioned. Upon obtaining an appropriate contrast spread, 0.5 mL of 0.5 % bupivacaine was injected. After observing the patient for 30-seconds, an additional 7 mL of 0.5% bupivacaine was slowly injected over 1.5-minutes for a total injection volume of 7.5 mL to achieve blockade of the C6 cervical sympathetic ganglion. The needle was withdrawn, and an adhesive bandage was placed on the injection site. This was followed by the superior cervical ganglion block (SCGB) technique again, fluoroscopy was used for needle placement. This time, the skin at the injection site on the lateral neck was anesthetized with 1 mL of 1% lidocaine. A 22-gauge 3.5-inch Quincke needle was inserted to a depth where contact was made with the ventrolateral aspect of the C3 vertebral body. The needle was pulled back 1 mm. Lateral view of the spine was obtained and the needle tip was confirmed to be dorsal to the ventral aspect of the patient was taken back to the recovery room and allowed to awaken. In the recovery room, 15-minutes post-procedure the patient was observed for facial anhidrosis and Horner’s syndrome symptoms (namely ptosis and miosis). Both before and after the procedure, the patient was informed as to possible life-threatening procedure-related adverse events and informed to urgently present to the emergency room if experiencing respiratory or cardiac issues. All patients tolerated the procedure well.
Psychometric Testing
The PTSD checklist score version DSM V (PCL-5). The primary outcome measurement for this study was the PCL-5 score. The PCL-5 is a 20-item self-reported questionnaire that assesses PTSD symptomatology based on 20 symptoms outlined in the DSM-5. The purposes of this test include screening, diagnosis, and monitoring of symptomatology over some time. The patient is to selfreport a score based on a 5-item Likert scale from 0 to 4, which is described by the following: 0) “Not at all”; 1) “A little bit”; 2) “Moderately”; 3) “Quite a bit”; and 4) “Extremely”. It should be noted that there are several differences between PCL-5 and PCL4 (based on DSM-IV), hence they can neither be compared nor interchanged. The total symptom severity is a sum of the patient responses and may range from 0 to 80.14
Patients with PTSD were included in the study if they had a pre-procedure PCL score of 31 or above. Patients had active PTSD and were seen in an interventional pain clinic for CSB. These patients were asked to complete a pre-procedure and postprocedure PCL-5 survey, as appropriate. Post-procedure PCL was obtained between 7 and 30-days post-intervention. PCL scores obtained were stratified by patient demographic and clinical information was collected, including age, gender, type of trauma leading to PTSD, history of suicidal attempts, and psychiatric medication use. Detailed informed consent was obtained before performing all procedures. Patients were allowed to elect to receive light sedation performed by a board-certified anesthesiologist. Exclusion criteria included PCL score <31, active suicidality, and having had a previous CSB treatment. The primary outcome measurement for this study was the PCL-5 score. A change in PCL-5 score by 5-10 points is considered reliable, and by 10-20 points is considered clinically significant. The optimally efficient minimum cutoff score
that is considered diagnostic ranges from 31 to 33.14 It is important to note that previous studies have demonstrated a strong correlation (0.929) of PCL with the Clinician Administered PTSD Scale (CAPS) diagnosis scale.15
Data Analysis
Statistical analysis was performed by Stella Center (Chicago, IL, USA), consisting of an independent samples t-test. Inferential tests were set at a 95% level of confidence (p<0.05).
RESULTS
A total of 99 patients who received right-sided CSB were collected for chart review and data analysis. Data included in the final analysis was obtained over the period of July 2021 through May 2023. All 99 patients included in the study were treatment naïve to CSB. The patient population consisted of 49 men and 50 women. Statistics regarding trauma type were recorded beginning in July 2022, which is why this data was collected for only 44 of the 99 subjects. We identified 22 types of self-reported trauma across these 44 subjects.
Patients
Group comparisons between genders for the mean change in PCL scores from pre- to post-intervention were performed with an independent samples t-test. Although the men had a slightly greater mean change in PCL scores (M=-23.69, SD=18.57), the results were not statistically significant when compared to women (M=- 21.64, SD=17.42; p=0.571).
When considering the data set as a whole, changes in PCL scores from pre- to post-intervention showed a drop greater than 10 points in 74.7% of patients (74/99), with an average change in PCL score of 22.66.
Trauma Type Categories
The trauma type categories are listed in Table 1 below (n=44). Comparative tests were not performed on the outcome of PCL score change between the trauma types because a patient could have been classified into more than one trauma type. Thus, the independence of groups was not assured.
| Table 1. Average Trauma Types Reported |
|
Reported Trauma Type
|
Responses |
% of Respondents
|
| Childhood trauma |
22
|
50.0%
|
| Personal health |
17
|
38.6%
|
| Witnessing violence |
16
|
36.4%
|
| Physical violence |
15
|
34.1%
|
| Bullying hazing |
14
|
31.8%
|
| Childhood sexuala assault |
13
|
29.5%
|
| Death of a loved one |
11
|
25.0%
|
| Other trauma |
10
|
22.7%
|
| Domestic abuse |
9
|
20.5%
|
| Workplace injury |
9
|
20.5%
|
| First responder |
8
|
18.2%
|
| Non-physical-interpersonal abuse |
8
|
18.2%
|
| Workplace abuse |
8 |
18.2%
|
| Divorce |
7
|
15.9%
|
| Loss of a pregnancy |
4
|
9.1%
|
| Adoption |
2
|
4.5%
|
| Combat/Warfare |
2
|
4.5%
|
| COVID |
2
|
4.5%
|
| Homelessness |
2 |
4.5%
|
| LGBTQ trauma |
1
|
2.3%
|
| Reproducted trauma |
1
|
2.3%
|
Safety and Patients’ Tolerability
Minor Adverse events included mild pain bruising at the injection site which resolved without treatment in three patients. One patient experienced an exacerbation of long-standing bipolar syndrome successfully addressed by re-engagement with a treating psychiatrist.
DISCUSSION
The purpose of this retrospective analysis was to determine the therapeutic benefit of CSB, which is SGB plus superior cervical ganglion block, on symptoms of PTSD in a cohort of Australian patients stratified by gender and types of inciting trauma. Additionally, while previous studies have primarily focused on American male patients with military-based trauma, our study demonstrates a similar impact on the widespread applications of CSB to the general Australian population with heterogeneous psychosocial backgrounds. The results of this study also show that CSB appears to be equally promising for women as well as men.
This is consistent with a larger published study by Dr. Lipov in 2022 based on 484 patients with 22 types of trauma.16
These findings suggest that the current guidelines for treating psychological Trauma in the Australian population may benefit from a fundamental change in approach by considering that psychological trauma may produce biological changes to the central nervous system, such as over-activation of the amygdala.17 Our results suggest that these physiological changes may be reversible following CSB and help resolve PTSD-related symptoms, currently recognized as psychological. Deactivation of the amygdala following SGB has been previously demonstrated.18 The exact physiological mechanism of CSB’s effect on the symptoms of PTSD currently remains unknown. A plausible theory of the mechanism of effect was postulated in 200911 based on experimental evidence.
In summary, a PTSD-causing event increases the nerve growth factor (NGF) in the cervical sympathetic ganglia, leading to intracranial sympathetic fibers sprouting that persistently mediate increased CSF norepinephrine (NE) levels. The increased NGF is needed for the maintenance of the sprouted sympathetic fibers. Local Anesthetic agents decrease NGF concentration in the cervical sympathetic ganglion, resulting in the pruning of sympathetic fibers, which leads to a reduction of NE and reduction of PTSD symptoms over a prolonged period.11
Synergistically targeting extra-cervical sympathetic ganglia has recently been shown to enhance the efficacy of SGB in the treatment of PTSD, especially in individuals who do not react to SGB alone.13 Since no sympathetic efferent fibers leave the cervical spinal cord, the sympathetic efferent fibers supplying the brain likely all originate from the thoracic spinal cord, primarily from T2 to T4, and ascend to the upper cervical ganglion through the stellate ganglion.19 This follows the logic that efferent sympathetic fibers from the thoracic ganglia often follow the vascular supply. In contrast to the superior cervical sympathetic ganglion, which travels down the internal carotid artery to the brain, the stellate ganglion sympathetic fibers follow the vertebral artery to the brain, according to Moore et al20. Both separately and together, those arteries supply various regions of the brain. So it stands to reason that a dual blockade of the sympathetic nervous system would result in a more intense effect on the brain, which would increase pruning and clinically result in a greater and more impactful reduction of PTSD symptoms.18
Ultimately, the current analysis suggests that the advancement of psychological trauma care may require a fundamental change in approach based on the discovery that trauma at its core is a biological injury that manifests with associated psychological changes. With CSB, this biological damage can directly be targeted. Finally, it is important to note that the effects of this treatment may be enhanced by working with qualified talk therapy professionals. A new standard of care for those who have experienced psychological trauma may be established as a result of the integration of medical innovation with best practices in talk therapy, resulting in longer, significant clinical improvements. The application of this strategy may broaden our comprehension of the trauma healing process and spur greatly needed innovation in the area of psychological trauma care.
LIMITATIONS
This is a retrospective cohort study. An RCT study would be significantly better. Such a study is being conducted utilizing functional magnetic resonance imaging (fMRI) at New York University (NYU). This was a retrospective study, the first of its kind, evaluating the efficacy of CSB in treating PTSD in Australian cohorts. These cohorts are what set this paper apart when studying PTSD. As such, limitations stem from the diverse patient selection, the limited scope of observation given the exclusive focus on preand post-PCL data, and the self-reported nature of the patientprovided data. Further, this report was limited due to inconsistent and short follow-up post-CSB, thus hindering the ability of this study to assess the duration of efficacy of CSB past the initial postprocedure assessment. Thus, generalizations from this study to a particular provider and cohort should be done with care.
CONCLUSION
Results of our retrospective cohort study suggest that regardless of the mechanism of trauma and multiple other factors presented, CSB appears to hold promise for both women and men, across a variety of traumatic experiences. This data set of 99 Australian patients, each treated by one of eight providers in one of four interventional pain clinics, adds to other studies suggesting that persistent over-activation of the sympathetic system has the potential for a reversal in a large percentage of patients by performing CSB. This is the first retrospective study that evaluated the efficacy of CSB for treating PTSD outside of the USA, which is where all previous case reports were conducted. All previous case reports and research related to CSB have been conducted on American cohorts. Thus, CSB seems to have a global level of implication in treating a disease as devastating as PTSD. This is a debilitating disease that does not discriminate based on age, gender, or location. A great deal of knowledge remains to be discovered, and research incorporating functional brain imaging of CSB as a PTSD treatment is required. However, CSB appears to be widely effective in relieving the debilitating symptoms of PTSD across a myriad of populations.
INSTITUTIONAL REVIEW BOARD PERMISSION
Given this is a retrospective study, the Institutional Review Board (IRB) for such study is exempted by the ethics committee. However, we will consider all the ethical and legal approvals in our followup CSB prospective study conducted at NYU.
CONSENT
Yes.
CONFLICTS OF INTEREST
Dr. Eugene Lipov is the Chief Medical Officer, Global of Stella, the practice who administered these treatments. Dr. Rob Wright is the Chief Medical Officer, Australia for Stella. Dr. Paul Verrills is a treating provider at Stella.


