INTRODUCTION
Obesity, overweight and physical inactivity are established causes for morbidity and mortality mainly because their direct association with several chronic diseases including diabetes, hypertension, hypercholesterolemia and coronary heart disease and cancer.1,2 Even though life expectancy has increased, especially in developed countries,3 obesity rates are still increasing and the CVD mortality is still over 17 million a year.3 Therefore, populations with a high CVD-risk require effective intervention strategies.
It is well known that the dietary habits improvement and physical activity are the most effective tools to prevent and reduce obesity and associated Cardiovascular disease (CVD), and then ultimately the mortality risk.4 However, when we consider high CVD risk populations, such as older, postmenopausal, obese patients and those with metabolic syndrome, a multi-disciplinary approach becomes essential for targeting the exercise and nutritional outcomes in order to ensure maximum CVD risk reduction and long-term adherence. Strategies based on a single approach, exercise or diet, have been demonstrated to be ineffective for ensuring long-term compliance and sustaining health benefits, particularly in reducing obesity related CVD cardiovascular risks.5 Therefore, this review introduces some recent evidence on the effectiveness of nutritional interventions combined with physical activity in order to reduce CVD risks in patients with high CVD risk.
Mediterranean Diet (MD) Effectiveness for Cardiovascular Disease Prevention
The various healthy dietary patterns often based on consuming healthy food components, such as diets found in Asian, Nordic, or Mediterranean regions present a nutritional effectiveness because the components act synergistically to reduce the risk of chronic diseases.6 One of the most popular, easy to follow, healthy dietary pattern, is the Mediterranean Diet (MD).7
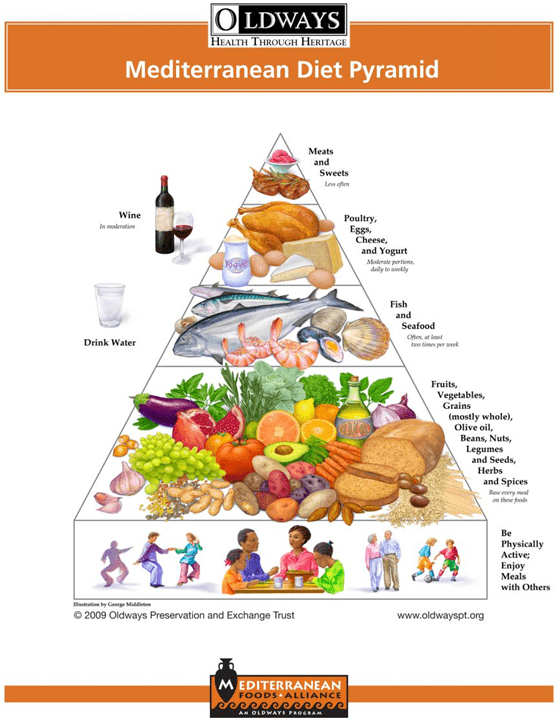
The MD is characterized by a high consumption of olive oil, fresh oily fish, legumes, fruits and vegetables, a moderate intake of dairy product and a low intake of meat as demonstrated by the MD food pyramid (Figure 1). The main cardioprotective MD components are monounsaturated fats such as oleic acid in olive oil, polyunsaturated fats such as Omega-3 (alpha-linolenic acid found in tree nuts such as Walnuts, Eicosapentaenoic acid found in oily fish), high amounts of flavoniods, antioxidants (found in fruits and vegetables), and high amount of fiber found mainly in cereal foods with a low Glycemic Index (GI).
Figure 1: Mediterranean Diet Pyramid (Oldways’s Pyramid Depiction of the Mediterranean Diet, www.oldwayspt.org)
There are several formulations about recommending the MD frequency of foods. Commonly accepted formulation for what constitutes MD foods has been reported as follows:8
– Olive Oil as added lipid
– Daily consumption of vegetables
– Daily consumption of fruits
– Daily consumption of unrefined cereals
– Bi-weekly consumption of legumes
– Nuts and olives as snacks (generally eaten just before a meal).
– Bi-weekly consumption of fish
– Daily consumption of cheese or yoghurt
– Monthly consumption of meat or meat products
– Daily moderate consumption of wine, if it is accepted by religion and social grounds
The MD has recently gained significant attention and many countries have adopted MD for their national CVD protection guidelines for, such as the NHS Healthy Choices in the UK or the Women’s Heart Foundation in the USA. Adopting MD nowadays is in line with the most recent research advances for reducing obesity-related CVD risk.9,10 Interestingly, adopting the MD seems to agree with the most recent research recommendations about the benefits of reduced high Glycemic Index (GI) carbohydrate type foods11 and increased consumption of “good fat” in the diet.12
Epidemiological and longitudinal intervention studies, based on primary or secondary CVD prevention strategies, have clearly shown that MD is associated with anti-atherogenic effects,7,13 reduced metabolic syndrome incidence, improved glycaemia control, low type-II diabetes incidence14,15,16 and decreased all-cause and cardiovascular mortality.13,14,15,16,17,18,19 The PREDIMED study20 has recently validated an effective tool to check the adherence to MD. This tool is based on a 14-Item Questionnaire (Table 1), and has been effectively applied in high-risk populations.21
| Table 1: Validated 14-item Questionnaire of Mediterranean diet adherence (based on Martinez-Gonzalez et al. 2012).21 |
|
Questions
|
Criteria for 1 point
|
| 1. Do you use olive oil as main culinary fat? |
Yes
|
| 2. How much olive oil do you consume in a given day (including oil used for frying, salads, out-of-house meals, etc.)? |
≥4 tbsp
|
| 3. How many vegetable servings do you consume per day? (1 serving: 200 g [consider side dishes as half a serving]) |
≥2 (≥1 portion raw or as a salad)
|
| 4. How many fruit units (including natural fruit juices) do you consume per day? |
≥3
|
| 5. How many servings of red meat, hamburger, or meat products (ham, sausage, etc.) do you consume per day? (1 serving: 100–150 g) |
<1
|
| 6. How many servings of butter, margarine, or cream do you consume per day? (1 serving: 12 g) |
<1
|
| 7. How many sweet or carbonated beverages do you drink per day? |
<1
|
| 8. How much wine do you drink per week? |
≥7 glasses
|
| 9. How many servings of legumes do you consume per week? (1 serving: 150 g) |
≥3
|
| 10. How many servings of fish or shellfish do you consume per week? (1 serving 100–150 g of fish or 4–5 units or 200 g of shellfish) |
≥3
|
| 11. How many times per week do you consume commercial sweets or pastries (not homemade), such as cakes, cookies, biscuits, orcustard? |
<3
|
| 12. How many servings of nuts (including peanuts) do you consume per week? (1 serving 30 g) |
≥3
|
| 13. Do you preferentially consume chicken, turkey, or rabbit meat instead of veal, pork, hamburger, or sausage? |
Yes
|
| 14. How many times per week do you consume vegetables, pasta, rice, or other dishes seasoned with sofrito (sauce made with tomatoand onion, leek, or garlic and simmered with olive oil)? |
≥2
|
Mediterranean diet and exercise interventions in high CVD risk populations
The analysis of the role of various MD components in cardiovascular risk reduction, including lipid profile, blood pressure control, inflammation and endothelial dysfunction, continues to be a challenge for both researchers and physicians. Recent evidence underlines the importance of olive oil fatty acids including oleic acid, phytosterols (Beta-sitosterol), antioxidant (alpha-tocopherol), and plant ployphenols in reducing inflammation, oxidation and determining improvements in endothelial micro- and macro-vascular function.22,23 Populations with high CVD risks such as older patients or patients with metabolic syndrome or postmenopausal women, seem to take particular advantage from this consumption.24,25,26 In particular, when those MD benefits are compared with to caloric restriction type diets.21 For example, it has been shown that following an MD supplemented with extra virgin olive oil and tree nuts is more effective than low fat diet for several anti-inflammatory effects such as reducing serum C-Reactive Protein (CRP), interleukin-6 (IL6) and endothelial and monocytary adhesion molecules, in a group of 516 high-risk men and women.22
In another study on men with metabolic syndrome, Richard et al. (2013)24 demonstrated that CRP, IL-6, IL-18 and tumor necrosis factor-α (TNF-α) have adapted differently when patients combined 5 week of MD with a weight loss program, compared MD without weight loss. In particular they demonstrated a 26% reduction in CRP concentrations and a 10% reduction in an arbitrary inflammatory score that included CRP, IL-6, IL-18, and TNF-α when the group followed MD only, while when a weight loss program was combined with MD, the reduction in the inflammatory markers was almost doubled for plasma IL-6 (-21%) and IL-18 (-15.6%) compared with the control diet, with no significant impact on plasma CRP concentration. More recent interventions have demonstrated a greater endothelial micovascular markers improvement in sedentary older adults and in postmenopausal women when moderate intensity exercise training regime was combined with MD for two months.25,27
These findings suggest that combining a healthy MD intervention with a weight loss or exercise training is more effective than MD and exercise or diet alone in maximising the risk reduction benefits, particularly when these treatments are targeted to high-risk groups, including individuals with the metabolic syndrome, older patients and postmenopausal women. Furthermore this evidence supports the importance of identifying sensitive biomarkers to detect the improvement in the endothelial vascular activity and to confirm the bioavailability of MD components and MD adherence, in order to distinguish the exercise and the MD health benefits.
In terms of the type of exercise, low to moderate exercise intensities in the aerobic intensity domain (below anaerobic threshold) are commonly associated with better long-term exercise compliance; particularly in obese and older populations.26 However, it is important to note that regardless of weight loss outcomes, achieving an improved cardiorespiratory capacity as a result of any exercise intervention is essential, because low cardiorespiratory fitness is considered as important as overweight and obesity as mortality predictor.2
A promising long-term compliance in a combined MD and exercise intervention has been recently reported in a follow-up study, one year after the initial 8 weeks of a program with MD and moderate-to-heavy intensity training (based on participants’ perception of exertion effort) in older sedentary, otherwise healthy participants.24 Sustained CVD risk reduction benefits were found after one year, particularly in microvascular endothelial function and cardiorespiratory capacity indicated by ventilatory thresholds, which may suggest that the moderate-to-heavy exercise intensity training is more appropriate when it is combined with an MD intervention.28 This suggestion is in agreement with recently reported positive effects of 12 weeks of moderate-to-heavy exercise training combined with MD29 on physical aspects (weight loss, physical function and improvement of metabolic syndrome risk factors) and mental domains of health related quality of life measures (vitality, general physical health, emotional role, and self-perception of health).
Similar cardiometabolic and microcirculatory adaptations have been demonstrated in healthy humans who followed a High Intensity Interval Training (HIIT) protocol in healthy and active adults,30,31 and more recently in healthy obese and metabolically unhealthy obese adults.32 In two groups of metabolically healthy and unhealthy obese older adults, Dalzil et al. (2014)32 applied a nutritional counselling based on MD, in addition to HITT protocol with a first follow up after 9 months. They reported similar cardiometabolic improvements in both obese groups in terms of body composition, BP, fasting glycemia, insulin sensitivity, peak oxygen uptake, and muscle endurance, suggesting similar clinical health benefits. However, due to the different cardiometabolic markers considered in the various studies, and the differences in the CVD risk scores, it remains uncertain whether the combination of MD and physical activity would be more effective or would produce a better long-term compliance compared with an MD or an exercise intervention alone.
Strength training is an important exercise strategy for preventing muscle loss, particularly in older population. Although limited research combined light strength type training with an MD intervention, and this combination seems to produce a good MD compliance.33 Talegawkar et al. (2012)33 reported an inverse association between age-related strength loss (measures of frailty) and the adherence to MD in community dwelling elderly men and women. Strength training may also provide postmenopausal related vascular improvement including adipose biomarkers of arterial stiffness.34 Therefore, it may be beneficial to combine MD with strength training in order to achieve vascular risk reduction outcomes in older (i.e. postmenopausal, frail) population groups. Longitudinal interventions combining MD with a variety of types of physical activity and exercise interventions (particularly HIIT and strength types) in high CVD risk groups and the related modifications of specific CVD risk biomarkers would certainly merit further research in future.
CONCLUSION
An effective dietary strategy must rely on a multi-faceted approach, particularly when targeting high-risk population such as older population. The increase in the age expectancy, is accompanied by risk of cardiovascular disease due to hormonal, metabolic and cardiorespiratory changes. Recent evidence on the combination of exercise interventions with MD demonstrated risk reduction benefits in cardiovascular disease markers including improvements in endothelial function, reduced inflammatory markers and improved cardiorespiratory and metabolic capacity in older patients, and in obese and metabolic syndrome patients. Combining MD with various physical activity and exercise training protocols included moderate aerobic, high-intensity interval training and strength training, have shown effectiveness in reversing the cardiovascular risk in a variety of high-risk populations. However, it is still unknown whether the specific benefits are attributable to exercise or MD and many other studies; furthermore the CVD risk reduction biomarkers, particularly endothelial and inflammatory biomarkers, would certainly merit further studies in future.
DISCLOSURES
No interest conflict.


