INTRODUCTION
Treatment of gonarthitis by closed wedge high tibial osteotomy is a widely applied method in practice of modern orthopaedics.1,2,3 Numerous scientific works, which recently appeared in the periodic literature, confirm both high interest to the given problem and efficiency of this method.4,5,6,7 The discussion deals basically with the choice of correct indications for the osteotomy, and also with selection of a method for its carrying out.
Currently, high tibial osteotomy is recognised as a confident alternative to total knee prosthesis. At first sight, total knee prosthesis is more advantageous. It has a short term of postoperative rehabilitation, and provides more precise positive outcome of the treatment. In contrast, the basic advantage of closed wedge high tibial osteotomy within the treatment of knee arthritis is the opportunity to maintain the function of natural knee joint. It is well documented that the choice of closed wedge high tibial osteotomy by correct management of its indications gives high density of successful results of treatment.4,5,6,7
By the combination of arthritis in the medial tibiofemoral compartment and varus deformations of the knee, the traditionally applied treatment is the closed wedge high tibial osteotomy through external access with osteosynthesis by staples.2,3 The limitations of the method are the necessity of postoperative immobilization, late term of loading and long period of functional recovery. Furthermore, it is necessary to note a small range of correction for the varus deformation. From different medical sources, the maximum of correction makes between 15 and 25°.2,3,4,7
The studies performed in our department on early loading after arthroscopy and total knee arthroplasty have forced us to reconsider the approach for postoperative rehabilitation after closed wedge high tibial osteotomy. The following study describes the effects of early loading after closed wedge high tibial osteotomy as the treatment of gonarthitis.
MATERIAL AND METHODS
The study included 37 patients, which were treated at our department by closed wedge high tibial osteotomy during the period between 1997 and 2004. All the patients were surveyed in dynamic. Thirty three were female and four male. As the indication for the operation was knee arthritis with primary lesion of the medial tibiofemoral compartment. A retrospective analysis of the treatment results of the patients was performed.
For the estimation of the joint condition a knee x-rays with functional loading (standing) were carried out prior to operative treatment. The roentgenograms formed a basis for planning and calculation of axis correction. Subsequently, operations were carried out under general anesthesia.
At the first stage, an arthroscopy checking joint surfaces, patella position, synovial capsule, presence of intraarthicular bodies, the condition of meniscuses and ligaments was performed and reasons for flex contracture were assessed. Removal of the intraarthicular bodies, partial resection of the meniscus, local synovectomy and fossa plastic were carried out for restoration of the full extension.
The operation using the external curved approach to the proximal tibia made the second stage. The osteotomy was performed by a chisel or oscillation saw according to the preoperative plan. The osteosynthesis was carried out using staples. For prevention of postoperative complications antibacterial prophylactic and Fraxiparin-forte for 14 days were applied.
According to the postoperative period two different groups of patients were allocated. The first group included 22 patients (two male and 20 female) in the age between 38 and 78 years who were operated during the period from 1997 till 2000. In this group isometric gymnastics began on the second postoperative day and immobilization was used within four weeks. The splint removal was followed by rehabilitation course. Partial weight bearing was allowed after 6th-8th and full bearing after 10th-12th postoperative week.
The second group included 15 patients (two male and 13 female) in the age between 42 and 68 years which were treated during the period from 2002 till 2004. The rehabilitation course in this group began also with isometric exercises on the second postoperative day and immobilization was used within two or four weeks. Partial weight bearing was allowed already after 3rd-5th postoperative day. Walking with a stick began after 4th-6th postoperative week depending on physical condition of the patient. As immobilisation, in two patients a brace was applied from 7th postoperative day. For all other patients a plaster cast was used during all period of fixation.
For the knee assessment at follow ups a standard “Knee Sosiety” scale was applied.8 For the estimation of the effect of early loading after the osteotomy the analysis of the postoperative period and, importantly, of the early complications were performed.
The short-term follow up for both groups was performed on the 4th postoperative month and one year after operation. The long-term follow-ups for the first group lay between 5th and 8th and for the second group between 1st and 3rd postoperative year. Statistical differences of the treatment results in the groups were assessed using Student’s t-test (two tailed, α=0.05).
RESULTS
In the first group of patients the estimation of the short-term results using the “Knee Sosiety” scale showed (on the average) following points combinations: preoperative – 98 points; 4th months follow up – 145 points and one year follow-up – 167 points. In the second group of patients comparable points combinations were documented: preoperative – 102 points; 4th months follow up – 167 points and one year follow up – 172 (Diagram 1) (Figure 1).
Diagram 1. The results of the treatment of patients using the “Knee Sosiety” score at the short-term follow ups.
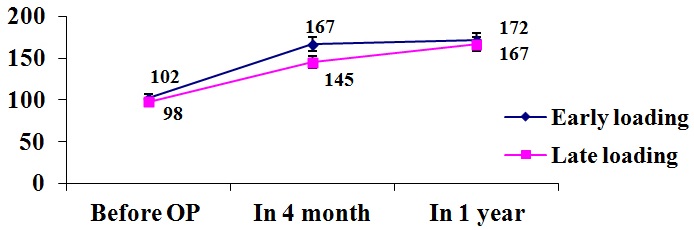
Figure 1. Case report: A 51-year-old male was treated using closed wedge high tibial osteotomy. Immobilization was 2 weeks. Partial weight bearing was allowed from the 3rd postoperative day.
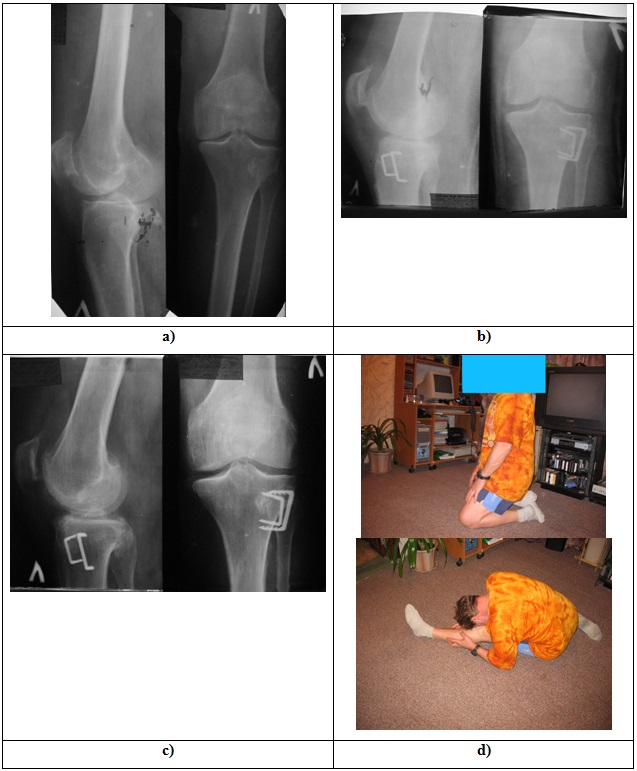
The images shows a) the preoperative x-ray; b) the x-ray performed at the second postoperative day; c) the x-ray carried out at the follow up of 8 years; d) the functional result of the patent at the 10 years follow up.
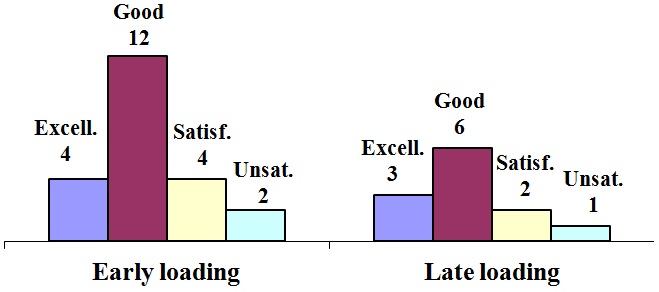
The long-term results of the treatment in the first group (late loading) of the patients were excellent in four, good in 12, satisfactory in four and unsatisfactory in two patients. The long-term results in the second group (early loading) of the patients were excellent in four, good in eight, satisfactory in two and unsatisfactory in one patient (Diagram 2) (Figure 1).
Diagram 2. The results of the treatment of patients using the “Knee Sosiety” score at the long-term follow-ups.
The comparative analysis of functional recovery in the first and second group of patients showed that early loading allowed for faster postoperative rehabilitation. This was confirmed by the computer system for gait analysis. This is also indicated by significantly different (p<0.05) results in the two groups at the 4 months follow up (Diagram 1).
The number of complications after operations in researched group of patients was not too large (Table 1). Significant differences in complications between the first and second group of patients were not seen (Table 1). Thus, application of early weight bearing after closed wedge high tibial osteotomy has not led to increase in the number of postoperative complications.
Table 1. The distribution of postoperative complications after closed wedge high tibial osteotomy between the two studied groups.
|
№
|
Complication
|
Late Loading
|
Early Loading
|
Total
|
|
1
|
Deep venous thrombosis |
1
|
1
|
2
|
|
2
|
Delayed union |
1
|
0
|
1
|
|
3
|
Recurrence of the varus deformations |
3
|
2
|
5
|
|
4
|
Total |
5
|
3
|
8
|
DISCUSSION
Currently, development of techniques and approaches for operative interventions in orthopaedics goes on the way of achievement of the shortest possible rehabilitation period, which is mainly due to the high hospital costs for patients stay.
The idea for this study was born after introduction of early full loading after total hip and knee arthroplastic in our clinic. This technique has been borrowed from our German colleagues, and it has repeatedly passed check, both on efficiency and on safety.9 Observing patients after total hip arthroplasty, we concluded that early loading does not slow down but accelerates process of functional recovery of the joint. Similarly, considering our experience with knee arthroscopy, which was initially, before 10 years, followed by late weight bearing on the 4th or even 10th postoperative day and currently is the subject of one day hospitalisation, an early loading is advantageous.
Additionally to these ideas, the other reason for this study was the fact that three of our patients have began with early loading without our advice and in contrary to our recommendations after they were discharged from the hospital (within the 2nd postoperative week). At the follow-up of the 4th postoperative week each of these patients showed a good range of motions and a good radiologically confirmed consolidation of the osteotomy.
The study was performed on two groups of patients with comparable age and sex distribution. The indication for the treatment of knee arthritis by closed wedge high tibial osteotomy was carefully examined in all patients.
Our short- and long-term results of the treatment in the both studied groups showed similar distribution of good and poor result without significant differences. This indicates that early weight bearing after high tibial osteotomy does not worsen process of rehabilitation and result of the treatment. In contrary, early loading allowed for faster postoperative functional recovery. The absence of statistical differences regarding postoperative complications indicates the safety of the approach.
In the presented study, the second group of patients, in which the early postoperative loading was applied, included 15 patients. Furthermore, long term follow ups for the groups were different. Although, in comparison with the group of late loading, good results of the treatment and even faster functional recovery of the patients with early loading was documented, further studies using the described rehabilitation approach are necessary.
In conclusion, based on our results we assumed that after closed wedge high tibial osteotomy the early postoperative loading is an advantageous rehabilitation approach in comparison with the late loading due to a faster functional recovery and a shortening of the patient hospitalisation. Nevertheless, further multi-patient studies on this approach with similar long-term follow ups are necessary.
CONFLICTS OF INTEREST
The authors have no conflicts of interest to declare.
CONSENT
The authours have obtain written informed consent from the patient for submission of this manuscript for publication.


