INTRODUCTION
Chikungunya (CHIK) is a disease caused by a mosquito-borne alphavirus, called the Chikungunya virus (CHIKV). It is found that CHIKV circulates in two distinct transmission cycles (enzootic transmission and urban transmission). The enzootic transmission occurs among nonhuman primates and perhaps other vertebrates by arboreal Aedes spp. mosquitoes in sub-Saharan African sylvatic foci. The urban transmission occurs in humans by Aedes mosquitoes (Aedes aegypti, Aedes albopictus).1,2 CHIKV is an enveloped, RNA positive-strand alphavirus belonging to the Togaviridae family.3
Figure 1 shows the relation between CHIK and the CHIKV, as well as, the forms of transmission by the Aedes mosquitoes. CHIKV is an African virus that circulates enzootically in a sylvatic cycle between arboreal, canopy-dwelling mosquitoes and non-human primates.2
Figure 1: Forms of transmission of the Chikungunya virus by the Aedes mosquitoes
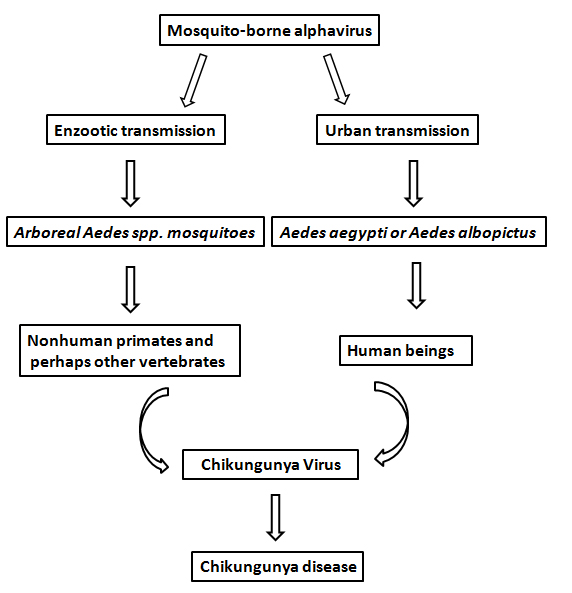
CHIKV is an African virus that circulates enzootically in a sylvatic cycle between arboreal, canopy-dwelling mosquitoes and non-human primates.2 CHIK is an endemic disease to many countries in Western, Central, Eastern and Southern Africa, Indian Ocean, West Pacific Islands and South-East Asia.1 Since 2004, CHIK has expanded its geographic range to Indian Ocean Islands, Italy, France, and America.1,2
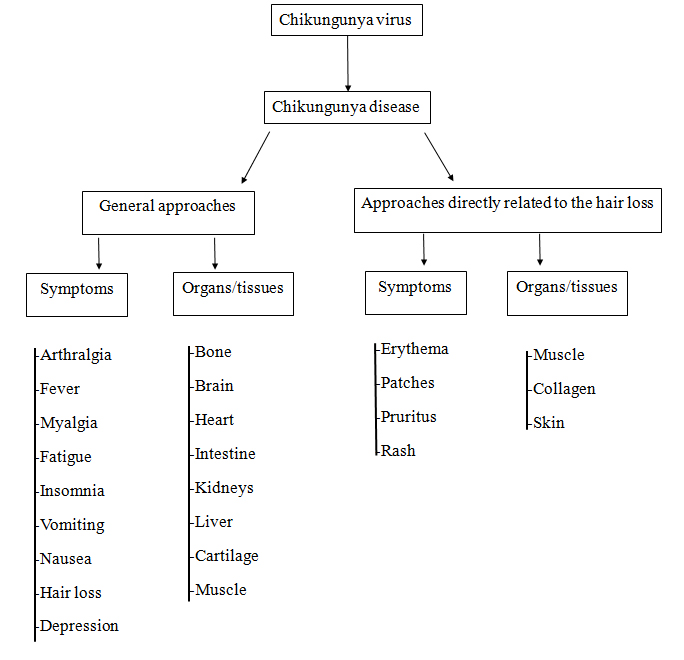
Despite several clinical symptoms being associated with CHIK,2,4 little attention is paid to scalp lesions in CHIKV infection that can lead to hair loss.4 This could be related to the fact that hair has no vital function in humans; although, it has important psychological functions that are recognizable in most people.5 However, in the field of alpha viral infections, hair loss is consistent with alopecia and was reported in an experimental model with mice.6 These symptoms related to CHIK are associated with several organs and tissues. Based on the study by Soumahoro et al4 (Figure 2), certain general symptoms as well as organs and tissues which could be affected by CHIK are mentioned. Also the clinical approaches associated with hair loss have been specified (Figure 2).
Figure 2: General Approaches of the Chikungunya Disease and the Hair Loss
Turner et al7 consider that hair is the ultimate personal beauty tool of self-expression. In addition, it is, in general, more malleable than skin and it is more personal than clothing. Hunt and McHale8 have described that alopecia is a chronic dermatological disorder in which hair fall occurs partly or completely from the areas such as the scalp or other parts of the body.
Based on the study by Hunt and McHale8 alopecia is considered as a chronic inflammatory disease that affects the hair follicles. It is neither life threatening nor painful; however, there can be irritation of the skin, as well as appearance related problems resulting from the loss of eyelashes and eyebrows. Alopecia can also be associated with serious psychological consequences, particularly in relation to anxiety and depression. Watras et al9 reported that hair loss might also be associated with the use of medications, such as anticoagulants. Different medications have been used for the treatment of CHIKV infections.10,11
Some factors associated with hair loss are found to be related to CHIK, as the CHIKV can target different human cells, such as epithelial and endothelial cells, fibroblasts and macrophages,12 HeLa cells13 and muscle progenitor cells.14 Therefore, CHIKV can be associated with clinical manifestations including rashes15–17 and urticaria.18 CHIKV could also damage collagen and matrix metalloproteinases (MMPs)19 and alter the connective tissue metabolism.20 In skeletal muscles, the atrophy and necrosis of scattered muscle fibers and the vacuolization of cells have also been shown to have potential to affect underlying mechanisms related to a disorder known as myositis syndrome.12 Putting together these findings, it is relevant to consider that if these phenomena can lead to degenerative chronic lesions, it is possible to say that the target human epithelial and endothelial cells, fibroblasts and macrophages,12 muscle progenitor cells,14 hypermelanosis, xerosis18 might cause a great variety of clinical manifestations including hair loss.4
Various authors21–23 have used databases, such as PubMed, to evaluate the scientific findings in this topic. PubMed is a database that comprises of more than 26 million citations for biomedical literature from MEDLINE, life sciences journals, and online books. Citations may include links to full-text content from PubMed Central and publisher websites. Several studies have utilized this database for revisions and investigations involving CHIK.21–23
The aim of this review is to present some symptoms related to CHIK and tissues and organs that are target to the CHIKV, leading to hair loss.
MATERIAL AND METHODS
Database used:
Two searches were performed through PubMed (http://www. ncbi.nlm.nih.gov/pubmed) database.
1. Search strategy used to verify the publications involving chikungunya and some symptoms associated with this disease caused by an arboviral alphavirus.
The searches were performed to verify the number of publications (NP) with the keywords, ”chikungunya and fever”, or “arthralgia”, or “rash”, or “myalgia”, or “fatigue”, or “depression”, or “insomnia”, or “pruritus”, or “patches”, “nausea”, or “vomiting”, or “headache”, or “erythema” or “hair loss”.
2. Search strategy used to verify the publications involving chikungunya and some organs or tissues that are target of the arboviral alphavirus associated with this disease.
The searches were performed to verify the NP with the keywords “chikungunya and heart”, or “liver”, or “kidneys”, or “intestines”, or “skin”, or “brain”, or “muscle”, or “bone”, or “cartilage” or “collagen”.
Three reviewers independently accessed both the bibliographical databases through the Universidade do Estado do Rio de Janeiro on January 5th 2017.
Inclusion and Exclusion criteria to select the publications: All the publications about chikungunya and “hair loss” that were found in the PubMed database were included in this narrative review.
RESULTS
Table 1 shows the number and the percentage of the publications related to Chikungunya, that is an endemic disease in some countries. It also shows the symptoms and percentage of each symptom recorded in the number of publications with this infection in the PubMed database. The total number of articles with the keyword ”Chikungunya” is 3,176. It is observed that fever is the most cited symptom and 50% of the publications are related to this symptom. Arthralgia and rashes are other disorders associated with Chikungunya as shown in a relevant number of articles. It is also observed that hair loss is also a symptom that would be associated with CHIKV infection; however, it is poorly studied, with only one publication in the PubMed database.
| Table 1: Number of the Publications Involving Chikungunya and some Symptoms and the Percentage of each Symptom Related to the Total Number of Publications with this Infection in the PubMed Database. |
|
Symptoms
|
Number of Publications
|
Percentage of the publications (%)
|
| Fever |
1611
|
50.72
|
| Arthralgia |
283
|
8.91
|
| Rash |
235
|
7.40
|
| Myalgia |
75
|
2.36
|
| Headache |
71
|
2.24
|
| Fatigue |
22
|
0.69
|
| Nausea |
22
|
0.69
|
| Vomiting |
21
|
0.66
|
| Depression |
14
|
0.44
|
| Patches |
8
|
0.25
|
| Erythema |
7
|
0.22
|
| Pruritus |
6
|
0.19
|
| Insomnia |
1
|
0.03
|
| “hair loss” |
1
|
0.03
|
Table 2 shows the number of the publications related to Chikungunya and some targets (organs or tissues) with its percentage related to the total number of publications. Here, it is observed that skin is the most cited organ, but with only 2.77% of the total of publications with Chikungunya. It is also verified that the number of studies with the association between Chikungunya and kidney are high too.
| Table 2: Number and Percentage of the Publications Involving Chikungunya and Some Targets (organs/tissues) to the Chikungunya Virus in the PubMed Database. |
|
Organ/tissues
|
Number of Publications
|
Percentage of the Publications (%)
|
| Skin |
88
|
2.77
|
| Kidney |
68
|
2.14
|
| Brain |
64
|
2.02
|
| Muscle |
49
|
1.54
|
| Bone |
29
|
0.91
|
| Liver |
22
|
0.69
|
| Heart |
9
|
0.28
|
| Intestine |
7
|
0.22
|
| Cartilage |
7
|
0.22
|
| Collagen |
4
|
0.13
|
DISCUSSION
Following the aim of this review and considering the number of publications in PubMed, (i) amongst the symptoms related to CHIK, fever is the most reported, whereas, arthralgia and rash have significant NP (ii) the main targets of CHIKV were found to be skin, kidney and brain. Very few publications have been found with CHIK and hair loss. These finding could be associated with the fact that the hair does not have a vital function in humans, as reported by Ramos-e-Silva et al.5 In this case, it is possible to say that hair loss could not be considered in the clinical evaluation of the patient with CHIK, although, Mirmirani,24 considers that the hair is one of the most defining aspects of human appearance. Moreover, hair loss may be idiopathic, and would be associated with a genetic predisposition, metabolic and hormonal abnormalities and aging.5,7
The basis for this symptom following CHIKV infection is not understood. It could simply reflect a non-specific symptom triggered by the acute febrile illness, as reported by Ramose-Silva et al5 after many systemic diseases. Although, various clinical symptoms have been associated with CHIK,2,4 little attention is paid to scalp lesions in CHIKV infection that can lead to the hair loss. Soumahoro et al4 reported a comparative study of longstanding disabilities owing to CHIKV infection. It was showed several subjective symptoms (arthralgia, myalgia, fatigue, depression, hair loss) reported by people infected by CHIKV.
According to Hunt and McHale,8 alopecia is an inflammatory disease that affects the hair follicles. This consideration could help to understand the findings presented in Table 1. The analysis of the results reported in Table 1 indicates possible symptoms that could contribute directly to hair loss, as well as rashes, pruritus, patches and erythema. Moreover, other symptoms, such as depression and insomnia could be also associated with alopecia. As the hair is not considered a vital structure in the human beings, hair loss could not be an essential question to be asked in the clinical evaluation of the individual with CHIK disease.
By analyzing the findings reported in Table 2, it is possible verify the importance of certain tissues in which, some alteration could lead to hair loss, as well as affect the skin, muscle and collagen. Authors have suggested that CHIKV can cause a wide range of clinical manifestations including rashes, hypermelanosis and xerosis16–18 that can further contribute to hair loss. Moreover, damaged collagen, altered connective tissue metabolism, degenerative chronic lesions by the CHIKV could also be related to alopecia.4,14,20 It is important to point out that medications could also sometimes promote hair loss, as reported by Yang et al25 in the treatment of chronic hepatitis.
As the CHIKV infection can target different types of human cells12,14 and lead to many injuries in the collagen, in the matrix metalloproteinases,19 in the connective tissue metabolism,20 in the skeletal muscles, degenerative chronic lesions related to inflammatory responses and the possible subsequent effect of immune activation could promote hair loss.
All the above findings, showing a relation between CHIKV infection and hair loss, are reinforced with experimental studies. Ziegler et al6 described that newborn mice inoculated subcutaneously with CHIKV showed signs of illness (lethargy, loss of balance and difficulty in walking, dragging of the hind limbs, and hair loss around the inoculation site on the back) 7-10 days after infection. Vanlandingham et al26 reported that O’nyong-nyong virus (ONNV) and CHIKV are closely related viruses in the Semliki Forest antigenic complex (family Togaviridae, genus Alphavirus), whereas Walker et al27 reported that mice that were inoculated with unadapted ONNV at 28-30 hours of age, developed a patchy alopecia on the 4th-7th post-inoculation day, which usually lasted 4-5 days.
The current review has certain limitations that must be considered in the interpretation of the findings. Firstly, it includes only the papers found in the PubMed database. In addition, the keywords used in the searches were related to the symptoms, tissues and organs and Chikungunya identified in Soumahoro et al4 Therefore, more revision with other databases and keywords would be instrumental.
CONCLUSION
In conclusion, despite the limitations, it can be stated that, fever and skin are the two highly emerging terms related to Chikungunya as observed in a large number of publications. Moreover, it was observed that the presence of various symptoms mentioned above could lead to alopecia in patients with Chikungunya. In addition, as hair does not have a vital function in humans, it is possible to conclude that hair loss cannot be considered in the clinical evaluation of the patient with CHIK. Hence, hair loss cannot be yet accounted as a symptom of Chikungunya.
ACKNOWLEDGMENTS
The authors thank the Brazilian Agencies (CNPq and FAPERJ) for the support.
CONFLICTS OF INTEREST
The authors declare no conflicts of interest.
AUTHORS’ CONTRIBUTION
DSC, LLPD, EOGA, RPCL, SP, DSM, IB, CAF, CF, GD, EF and MBF participated in the elaboration and execution of the study. DSC, LLPD and EOGA accessed the bibliographical database. All the authors analyzed and discussed the data of the study. DSC, LLPD and MBF wrote the manuscript. EOGA, RPCL, DSM, IB, CAF, CF, GD and MBF reviewed the final version of the manuscript. All the authors read and approved the final version of this investigation.


