INTRODUCTION
Patient-care providers working in psychiatric hospitals are frequently exposed to verbal threats of violence and at times experience physical attacks resulting in post-traumatic stress.1,2 In addition, it is not uncommon for them to witness violence between patients or towards other staff members. The stress associated with the latter is known as secondary traumatic stress.3 Aside from these types of traumatic stress; emotional exhaustion, cynicism, and a reduced experience of personal accomplishment have also been observed in individuals working in stressful environments over a significant period of time. These symptoms are often referred to as burnout.4,5
This study is a re-analysis of the data from an earlier study to examine the predictors of burnout in psychiatric hospital patient care providers.2 The research question in the original study was related to the prevalence of post-traumatic stress symptoms (PTSS) in psychiatric hospital care workers and their relationships to resilience, compassion satisfaction, secondary traumatic stress and burnout.2 PTSS are symptoms of post-traumatic stress disorder (PTSD) that may or may not reach the level of a clinical diagnosis of PTSD. The findings of the previous study indicated that burnout was the strongest predictor of symptoms of PTSS. In addition, resilience was not found to have been significantly correlated to PTSS, contrary to much of the published literature.That finding led the author of this article to explore burnout with respect to psychiatric hospital clinical staff, and explore the possibility that resilience is a mediating factor in predicting burnout.
PUBLISHED RESEARCH ON THE RELATIONSHIP BETWEEN BURNOUT AND RESILIENCE
Burnout is conceptualized as an untoward phenomenon among workers in the human services field. It is characterized by three dimensions: emotional exhaustion, feelings of depersonalization or a lack of feeling towards recipients, and a limitation in one’s sense of personal accomplishment relative to their work.6 Resilience is the term frequently used to refer to an individual’s ability to persevere with respect to a particular adverse situation. Resilience is generally perceived as existing on a spectrum with different individuals having different abilities to ward off stress.7
An online literature search was conducted in June, 2018 using Medline. The keywords burnout and resilience were entered. Three hundred and eighty nine citations were found. Of those, 14 consisted of a meta-analysis, and cross-sectional or control trial studies, and are reported as follows.
A meta-analysis by Kyoung and Min8 examined 15 studies where burnout was measured. They observed that age and work setting were the two significant correlates related to burnout. However, none of the studies in their meta-analysis measured resilience.8
Four studies were found that examined burnout and resilience as the main variables and observed a significant correlation.9,10,11,12 Four additional studies identified both resilience and post-traumatic stress disorder or secondary traumatic stress disorder as factors that were significantly related to burnout.13,14,15,16
Treglown, et al17 found resilience to have a mediation effect with respect to burnout. Using structural equation modeling in a sample of 450 female ambulance personnel, they found that there are specific qualities within resilience (boldness and excitability) that either moderate (enhance) vulnerability or mediate (limit) it.17 Similarly, resilience was found to be a mediator with respect to burnout in three additional studies.18,19,20 Finally, one study observed that psychological empowerment mediated the relationship between resilience and burnout.21 Based on this brief review of literature, there is ample evidence to anticipate that resilience has a role in predicting burnout in a variety of populations, but none were psychiatric hospital care-givers.
METHODS
The original study on which this analysis is based employed a cross-sectional correlational design utilizing a sample of care-givers in a psychiatric hospital in the Northeast region of the US. The study was approved by the principal investigator’s university’s Institutional Review Board (IRB) and the hospital’s research committee. The participants were nurses, psychiatric aides, masters-level therapists/counselors, and psychiatrists. The care providers were recruited to the study by two university-affiliated research assistants, under the guidance of the principal investigator (PI). Confidentiality of the data was maintained by not requesting personal identifiers among the survey’s questions, and having the participants place their completed surveys into a sealed envelope that they then dropped into a locked box in the possession of the research assistants for which only the PI possessed the key.
The sample consisted of 172 participants out of the total of 250 patient care workers employed by the hospital (69% return rate). Nine (9) out of 172 collected surveys (5.2%) exhibited completely missing data on the dependent variable (burnout), and 14 additional cases were removed during the data cleaning process in order to eliminate outliers (2.5 standard deviations above/below the mean) related to the main independent variable (resilience).22 A pattern of non-random missing data was not observed, and none of the standardized scales had partially missing data. As a result, replacement of data was not needed. The sample that was analyzed consisted of N=149 cases. See table 1 for the descriptive characteristics of the sample.
| Table 1. Demographic Characteristics of the Sample |
|
|
Category
|
% |
N |
| Title |
RN |
32.3 |
|
|
Psychiatric Aide
|
40.5 |
|
| Assistant Counselor |
6.3
|
|
|
MD
|
2.5 |
|
| Case Coordinator |
7.0
|
|
|
Therapeutic Rehab
|
1.3 |
|
| Other |
10.1
|
|
|
Total
|
100 |
158 |
| Shift |
Day |
847.2 |
|
|
Evening
|
28.0 |
|
| Night |
24.8
|
|
|
Total
|
100 |
161 |
| Age (years) |
<21 |
0.6
|
|
|
21-30
|
36.1 |
|
| 31-40 |
18.3
|
|
|
41-50
|
20.7 |
|
| 51+ |
24.3
|
|
|
Total
|
|
169 |
| Gender |
Male |
33.1 |
|
|
Female
|
66.9 |
|
| Total |
|
172
|
|
Support
|
Married
|
51.9 |
|
| Live-in Partner |
9.3
|
|
|
Lives with Family
|
24.7 |
|
| Lives Alone |
14.2
|
|
|
Total
|
|
162
|
|
Race
|
African American
|
29.6 |
|
| Asian |
0.6
|
|
|
Caribbean
|
13.6 |
|
| Pacific Islander |
1.2
|
|
|
Latino
|
6.5 |
|
| White |
42.0
|
|
|
Total
|
|
169 |
| 8 Years of
Experience |
<1 |
7 |
|
|
1-2
|
20.3 |
|
| 3-4 |
22.7
|
|
|
5+
|
49.4 |
|
| Total |
|
172
|
|
Highest Education Attained
|
High School
|
13.4 |
|
| 1-3 years of college |
43.6
|
|
|
Bachelors
|
27.3 |
|
| Masters |
13.4
|
|
|
Doctorate
|
2.3 |
|
| Total |
|
172
|
MEASURES
To better understand the relationship of resilience and burnout, a number of other variables based on the findings in the original study were analyzed. They are: a) secondary traumatic stress symptoms, b) compassion satisfaction, c) confidence in coping with patient aggression, d) post-traumatic stress symptoms, e) the rates of traumatic events (TE’s; assaults & personal injuries), f) length of time since the last trauma-informed care meeting, g) length of time since the last violence management training session, h) non-workplace traumatic life events, and i) demographic statistics.
Burnout was measured using a standardized 10-item subscale of the Professional Quality of Life Scale (ProQol) called the Burnout scale (BO),23 and resilience was measured by the 14-item Resilience Scale (RS-14).24 The BO Scale is one of three standardized subscales of the ProQol scale, each with established reliability and validity. The other two subscales of the ProQol were also used to collect data in the study. They are the Secondary Traumatic Stress scale (STS)23,25 and the Compassion Satisfaction scale (CS).23
Standardized measures for other variables that were considered to be potentially related to burnout were the Confidence in Coping with Patient AggressionIndex (CCPAI),26 the Life Events Checklist,27,28 and the Post-traumatic Stress Checklist–civilian version (PCL-c).29,30 The published inter-item reliabilities of the standardized tools used to measure the study variables are identified in Table 2.
| Table 2. Published Alphas Coefficients of Standardized Tools Used |
|
|
Variable
|
Measure |
Alpha
Coefficients |
Reference
|
| Burnout |
BO
|
0.75 |
23
|
| Resilience |
RS-14
|
0.72-0.94 |
24
|
| Secondary Traumatic Stress |
STS
|
0.78-0.85 |
25
|
| Compassion Satisfaction |
CS
|
0.88 |
23
|
| Confidence in Coping with
Patient Aggression |
CCPAI
|
0.92 |
26
|
| Post-Traumatic Stress Symptoms |
PCL-c
|
0.85-0.94 |
29
|
| Life Events Checklist |
LEC
|
0.84-0.93 |
27
|
The number of workplace traumatic events (TEs; verbal abuse, threats and physical attacks) experienced by the participants was obtained through a series of researcher-developed questions as part of the demographic questionnaire. Twelve (12) categories of traumatic events (TE’s) were examined. Of the 12, four were different types of TE’s (verbal abuse, verbal threat, physical attack, & severe physical attack), each within one of three timespans (past 30 days, past 6 months and lifetime). The frequencies were recalculated during data entry to account for overlap among the time spans.
RESEARCH QUESTION AND HYPOTHESES
To understand burnout within this population, the study’s research question was: Does resilience act as a mediator with respect to one or more factors that are significantly related to burnout in a sample of psychiatric hospital care-givers? As a result, three hypotheses were formulated and tested based on mediation analysis methodology.22
Hypothesis 1: At least one of the following variables is significantly related to burnout: traumatic events, post-traumatic stress symptoms, secondary traumatic stress symptoms, compassion satisfaction, non-workplace traumatic life events (life events), or confidence in coping with patient aggression.
Hypothesis 2: Resilience is significantly related to burnout, while controlling for all other significant factors.
Hypothesis 3: Resilience acts as a mediator in at least one of the significant relationships related toburnout identified in hypothesis 1.
STATISTICAL ANALYSES
The following preliminary procedures were conducted. The level of significance (alpha) for all of the analyses that were conducted was set at 0.05. The RS-14 and BO scores were tested for normality. The descriptive statistics (mean, median, standard deviation and skew) for the BO and RS-14 scales suggested that the BO scores evidenced a satisfactory distribution of the data to permit the use of parametric tests (for normal distributions), but that the RS-14 scores evidenced outliers and required cleaning of the data in order to use parametric tests. As a consequence, 14 (7.6%) of the cases were deleted which facilitated the distribution achieving sufficient normality, resulting in N=149. See table 3 for a partial list of the psychometric properties of the data pertaining to the standardized measures.
| Table 3. Some Psychometric Properties of the Standardized Scales |
|
Variable
|
N |
M |
Mdn |
SD |
α |
Skew |
| BO |
163 |
20.68 |
21.00 |
5.02 |
0.72 |
0.09
|
|
RS-14
|
149 |
86.46 |
88.00 |
9.98 |
0.77 |
-1.14 |
| STS |
163 |
19.70 |
19.00 |
4.44 |
0.73 |
0.40
|
|
CS
|
163 |
41.03 |
41.00 |
6.97 |
0.74 |
-0.03 |
| CCPAI |
164 |
74.02 |
75.00 |
20.14 |
0.78 |
-0.192
|
|
PCL-c
|
164 |
25.29 |
22.00 |
9.09 |
0.76 |
1.39
|
| Note: The variation in sample size is due to cases not completing a
particular scale, except for the RS-14 which was cleaned of outliers and reduced by 14 cases. |
A Post hoc Power Analysis was conducted to determine the risk of a Type II error. Power was measured using G*Power 3.1 for linear regression analysis, a medium effect size, alpha=0.05, N=149 (RS-14 results), and 5 predictors. Power was predicted at 0.98 suggesting an adequate sample size to observe meaningful relationships among the factors.
For the purpose of identifying sample selection bias with respect to the dependent variable (BO), those scores were compared to each of the demographic variables to observe for significant relationships using the Independent Samples t-Test and ANOVA. Significant relationships between BO scores and demographic variables were not found.
RESULTS
Hypothesis 1:
TEs, PCL-c, STS, LEC, CS, or CCPAI is significantly related to BO.
The purpose of this hypothesis was to determine which of the measured factors (other than resilience) significantly interact with burnout. The frequency of each type of TE, and the scores for PCL-c, STS, LEC, CS, and CCPAI were analyzed for significant relationships with BO using Pearson correlation coefficients. Significant relationships were observed for all except one type of TE (physical attack in the past month) and LEC scores. Thus, these two variables were excluded from subsequent analyses. However, significant correlations were observed among the scores of all of the standardized scales, necessitating the use of regression analyses in order to control for multicollinearity.31 See table 4 for the significant correlations between BO and TEs, PCL-c, STS, CS, and CCPAI scores.
| Table 4. Pearson Correlation Coefficients for Variables Significantly Related to BO Scores |
|
Variable
|
Correlation Coefficient
|
| Verbal abuse, past month |
0.19*
|
| Verbal abuse. past 6 months |
0.30**
|
| Verbal abuse, lifetime |
0.30**
|
| Verbal threats, past 6 months |
0.27**
|
| Verbal threats, lifetime |
0.18*
|
| Physical attack, past month |
0.29**
|
| Physical attack, past 6 months |
0.38**
|
| Physical attack, lifetime |
0.23**
|
| Severe physical attack, past month |
0.25**
|
| Severe physical attack, past 6 months |
0.23**
|
| Severe physical attack, lifetime |
0.26**
|
| RS-14 |
-0.46**
|
| CCPAI |
-0.19*
|
| PCL-c |
0.41**
|
| CS |
-0.51**
|
| STS |
0.58**
|
| * p<0.05; ** p<0.01 |
|
Due to significant inter-correlations among the 11 categories of TE frequencies, the TE statistics were entered into a simple linear regression analysis as a single block and regressed against BO scores. None of the individual TE statistics was found to be significantly related to BO scores, when controlling for the other TE statistics. However, the TE statistics as a whole (the block of variables) was found to be significantly related to BO scores, F(12, 106)=56.630, p=0.005, R2=0.250, adjusted R2=0.14. As a result, BO scores were adjusted for TEs by entering the block of TE statistics in all of the following analyses.
Next, a series of five multiple linear regression analyses were performed (one for each of the variables found in the analyses associated with hypothesis 1 to be significantly correlated with BO, i.e., TEs, PCL-c, STS, CS & CCPAI). Each analysis consisted of 2 models with model 1 containing all of the control variables, i.e., those variables found to have been significantly correlated with BO except for the predictor variable (factor of interest) being analyzed, and model 2 consisting of the addition of the predictor variable. As a result, only PCL-c, STS and CS were found to be significantly related to BO when controlling for other significant variables.
In this series of analyses, CCPAI scores were not found to be significantly related to BO, and as previously reported, individual categories of TEs were not observed to be significantly related to BO. With respect to the latter, the frequencies of TEs, although a significant and robust factor related to BO, were ineligible in subsequent analyses as a predictor variable due to the inability to derive a reliable regression β coefficient. Therefore, the block of TEs was used as control variables in subsequent analyses in order to avoid their affecting the analyses of the relationships of BO and the other significant factors. The results are displayed in Table 5.
| Table 5. Multivariate Linear Regression Analyses of BO using TEs, PCL-c, STS, CS and CCPAI |
|
Predictor
|
TEsb |
PCL-cb |
STSb |
CSb |
CCPAIb |
| ΔR2 |
β |
ΔR2 |
β |
ΔR2 |
β |
ΔR2 |
β |
ΔR2 |
β
|
| Step 1 |
|
Control variablesa
|
0.51** |
— |
0.63** |
— |
0.61** |
— |
0.62** |
— |
0.64** |
—
|
| Step 2 |
|
Predictorb
|
0.14* |
NA |
0.02* |
0.19* |
0.04** |
0.30** |
0.03** |
-0.23* |
ns |
ns
|
|
Total R2
|
0.65** |
|
0.65** |
|
0.65** |
|
0.65** |
|
0.65**
|
|
| N |
163
|
|
163 |
|
163 |
|
163 |
|
163 |
|
| aControl variables include all variables related to BO at p<0.05, e.g., TEs, PCL-c, STS, CS, CCPAI and RS-14 (excluding the predictor variable for that specific regression)
*p<0.05, **p<0.01
NA: The TEs were entered as a block and do not have an individual beta.
ns: non-significant |
Hypothesis 2:
RS-14 is significantly related to BO while controlling for other significant factors.
The purpose of this hypothesis was to determine the extent to which burnout might be predicted by resilience. Multiple linear regression analyses were performed consisting of 2 models. In model 1, all of the variables previously found to be significantly correlated with BO, except for RS-14, were loaded and regressed against BO. These were considered the control variables in this analysis. In model 2, RS-14 was added to the analysis. The results indicate that RS-14 is a weak but significant inversely correlated variable with respect to BO, F(1, 99)=10.077, p=0.002, R2=0.043, adjusted R2=0.046, B coefficient=-0.146 (SE=0.046), β=-0.19, tolerance=0.616. In the analyses associated with this hypothesis, the total variance explained with respect to burnout was 65.1% (including the control variables). Resilience only explained 4.3% of that variance. See table 6 for the results of each of the steps of the hierarchical regression analysis for this hypothesis.
| Table 6. Multivariate Linear Regression Analyses Predicting Burnout from Resilience |
|
Predictor
|
ΔR2 |
B
|
| Step 1 |
0.609**
|
|
|
Control variablesa
|
|
|
| Step 2 |
0.042*
|
|
|
RS-14
|
|
-0.264*
|
| Total R2 |
0.651**
|
|
| n |
99
|
|
| aControl variables included TEs, STS, PCL-c, CS, CCPAI
*p<0.01, **p<0.001 |
Hypothesis 3:
Resilience acted as a mediator in at least one of the significant relationships related to burnout identified in hypothesis 1, i.e., PCL-c, STS and CS.
To analyze this hypothesis, three sets of multiple linear regression analyses were performed, one set for each of the significant predictors. Each set of analyses consisted of 3 models. In model 1, the control variables plus the predictor being analyzed were loaded (excluded RS-14) using BO as the outcome variable. This allowed for the determination of the β coefficient for the relationship between the predictor being analyzed and the outcome variable, excluding the effect of resilience. In model 2, the predictor was regressed against RS-14, using the control variables (excluding BO) as co-variates. This was necessary to determine the β coefficient for the relationship of the predictor and RS-14. Finally in model 3, the predictor and RS-14 were jointly regressed against BO, using the control variables as co-variates.22
The purpose of this last analysis was to determine the effect on the predictor β coefficient with the addition of RS-14 as a second predictor (mediation effect). If the β coefficient changed while remaining significant, then the supposition that RS-14 mediated the relationship between burnout and the predictor being analyzed is supported. In each of the analyses between RS-14 and PCL-c, STS, CS, and CCPAI, the relationships were not found to be statistically significant with a range of p-values from 0.136 to 0.663. As a result, it was concluded that RS-14 did not mediate any of the other predictors of BO.
Post hoc Analyses to Determine Relationships Among the Predictors: Path Analysis
To better understand the relationships of variables significantly related to BO, a path analysis was performed. A path analysis is a series of regression analyses that examine the relationships among variables based on theorized directionality; that is, one variable predicting the next.22 For the purpose of performing a path analysis, additional multiple linear regression analyses were performed to identify significant relationships among the predictors (excluding BO). Four simple linear regression analyses were conducted, each one using a different predictor as the outcome variable and the remaining predictors as independent variables. Three findings were significant. They are the relationships of the: 1) effect of RS-14 on CS, p<0.001, β=0.335, tolerance=0.749; 2) effect of STS on PCL-c, p<0.001, β=0.508, tolerance=0.959; and 3) effect of CCPAI on RS-14, p<0.001, β=0.451, tolerance=0.827.
Due to these interactions, mediation analysis22 was conducted to determine the effect of PCL-c with respect to the relationship of STS and BO (relationship series 1) and the effect of CS with respect to the relationship of RS-14 and BO (relationship series 2). The basic methodology for the analysis followed that outlined above in the section associated with hypothesis 3. The results indicated that PCL-c mediates the relationship of STS and BO (Aoian Z(STS/PCL-c–BO)=2.143, p=0.032; 23.5% of the effect of STS on BO is mediated through PCL-c) and CS mediates the relationship of RS-14 and BO (Aoian Z(RS-14/CS–BO)=-2.329, p=0.015; 25.98% of the effect of RS-14 on BO is mediated through CS.22 In addition, it was observed that the PCL-c and STS scores explained 14.4% of the variance with respect to BO, while CS and RS-14 scores similarly explain 9.5% of the variance. The results are displayed in Table 7.
| Table 7. Mediation Analyses Predicting the Effect of PCL-c on the Relationship of STS and BO, and the Effect of CS on the Relationship of RS-14 and BO |
|
Model
|
STS / PCL-c — BO |
Model |
RS-14 / CS — BO |
| ΔR2 |
β |
ΔR2 |
β
|
| 1 |
0.123**
|
|
1
|
0.058**
|
|
| BO predicted by STS |
|
0.407**
|
BO predicted by RS-14
|
|
-0.303**
|
| 2 |
0.240**
|
|
2
|
0.084**
|
|
| PCL-c predicted by STS |
|
0.508**
|
CS predicted by RS-14 |
|
0.335**
|
| 3 |
0.144**
|
|
3 |
0.095**
|
|
| BO predicted by STS |
|
0.298** |
BO predicted by RS-14 |
|
-0.264**
|
| PCL-c |
|
0.188*
|
CS |
|
-0.235**
|
| N |
99
|
|
N |
99
|
|
| Note: The mediation effect was tested using the Aoian Test.22
AoianZ(STS / PCL-c–BO)=2.143, p=0.032, 23.5% of the effect of STS on BO is mediated through PCL-c; Z(RS-14/CS – BO)=-2.329, p=0.015, 25.98% of the effect of RS-14 on BO is mediated through CS.
*p<0.05, **p<0.01 |
DISCUSSION
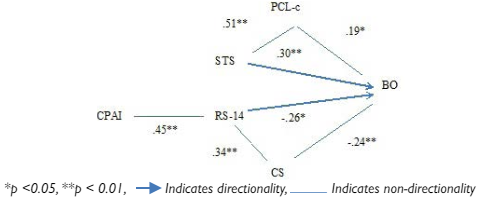
In summary, five of the studied factors were found to be significantly related to burnout i.e., aggregated TEs, PTSS, STS, CS and RS-14. Combined, they explained 65% of the variance related to burnout. However, each was a weak predictor with an R2 of less than 5%, except for aggregated TEs (R2=14%). Resilience was not found to mediate any of these relationships. However, a mediation analysis found that post-traumatic stress symptoms (PCL-c) mediated the relationship of secondary traumatic stress (STS) and burnout (BO), identified in this study as relationship series 1; also, compassion satisfaction (CS) mediated the relationship of resilience (RS-14) and burnout (BO), identified as relationship series 2. In other words, thepath analysis observed that trauma and stress are related to burnout in a separate set of relationships than resilience and compassion satisfaction (Figure 1). Please note that the relationships among the variables in Figure 1 depicted by arrows indicate theoretical causality based on the findings of previously published literature, whereas simple lines indicate correlation without the presumption of causality.
Figure 1. Diagram of the Path Analysis indicating the Beta Coefficients depicting the Effect of Confidence in Coping with Patient Aggression, Post-Traumatic Stress, Secondary Traumatic Stress, Resilience and Compassion Satisfaction on Burnout
Effect of Trauma and Stress on Burnout (Relationship Series 1)
The relationship between PTSD on burnout is well represented in the literature, and as a result will not be a focus of this discussion.32,33,34,35 Instead, the focus will primarily be on the relationship of resilience and burnout.
Effect of Resilience on Burnout (Relationship Series 2)
In this study, resilience was observed to have an inverse relationship with burnout and a direct relationship with compassion satisfaction, but it was not significantly correlated with STS or PTSS and did not act as a mediator with respect to PTSS, STS and burnout. This non-significant relationship with respect to resilience, trauma and burnout is similar to the results of a multi-site study that analyzed the same relationships in addition to coping styles in 298 pediatric physicians, nurses and nursing assistants in 9 hospitals.16 In that study, which also used path analysis methodology, it was found that coping style was the best predictor of burnout, and resilience did not remain significantly correlated with burnout or PTSD when controlling for other variables. These findings are similar to this study in that the relationship between resilience and burnout was affected by personality factors, i.e., coping style and compassion satisfaction.
Similarly, Treglown and others observed that resilience mediates the relationship between personality traits and burnout.17 This is similar to the findings of the present study in that resilience and a personality characteristic (e.g., compassion satisfaction) were related to burnout. However, the current study did not find that resilience was the mediating factor. Analytically speaking, it is possible that the difference in results could be due to compassion satisfaction being more highly correlated with burnout than the personality factors measured in the Treglown et al study.17
In a study of 70 disaster behavioral health responders comparing Compassion Fatigue (CF; a composite statistic based on BO and STS scores), resilience, compassion satisfaction, response to stressful events and burnout, resilience was observed to act as a mediator between compassion fatigue and burnout.23,36 In the current study, BO and STS were not combined to formulate CF. It is possible that the difference in results between the two studies is due to the manner in which the variables were treated or the differences in the sample sizes. It is also possible that the collinearity between CF and BO is high since CF is in part comprised of BO scores. In fact, a meta-analysis of studies of STS and BO did observe more robust correlations among those that utilized the CF framework than those studies that employed other measures.3 Since Burnett et al36 did not report the tolerance of these two variables (STS and BO), it is difficult to compare the results of their study to this one.
A number of other studies also examined the role of resilience and burnout, but none contained all three variables, i.e., PTSD or secondary traumatic stress symptoms, resilience, and burnout. So, it is difficult to validate the finding that there are two separate paths (identified in this study as relationship series 1 and 2) with respect to burnout. Most of these other studies observed that resilience appears to act as a mediator between burnout and personality traits or general health. In a study of 52 critical care nurses, resilience was observed to be a mediator between constructs of burnout (2 of 3 burnout subscale scores) and mental health.18 Similar results were observed by García-Izquierdo et al in a study of 537 nurses with respect to the mediating effect of resilience on the relationship of burnout and health.19 Finally, a study of 696 nurses observed the mediating effect of resilience on burnout in relation to workplace incivility.20 In summary, the literature on the relationships of resilience, stress/trauma and burnout is too limited to draw conclusions or to be able to adequately validate the findings of this study.
Resilience Scores in this Study Compared to Other Research
With respect to the non-significant relationship between resilience and PTSS or STS, one possibility is that the resilience of the sample was inadequate to have a protective effect or that the range of scores was too narrow. To determine the likelihood of this situation, the RS-14 scores in this study were compared to similar statistics in published literature that used the same scale. The mean and standard deviation for RS-14 scores in this study were observed to be 86.46 (SD=9.98). In other studies, RS-14 standard deviations were similar and the mean scores were lower, but probably not likely to be significantly so. In primary care physicians, the RS-14 scores were found to range from 79.9 to 83.2, but the standard deviations were not reported.37 Similarly, scores ranged from 74.88 (SD=17.05)38 to 62.80 (SD=10.13)36 in a sample of college students and 76.60 (SD=14.48)39 in a sample of adolescents. The overall similarity in scores adds to the validity of the resilience scores in this study and suggests that the lack of a significant mediator effect of resilience on the relationship of trauma/stress and burnout is probably not due to inadequate resilience in the sample.
BO Scores in this Study Compared to Other Research
BO scores in this sample were observed to have a mean of 21.0 and a standard deviation of 5.02. Other studies of psychiatric hospital nursing staff indicated means (standard deviations) as follows: 25.07(0.94),40 and 17.3(4.4).41 This suggests that the scores of this study’s sample were probably in line with other samples of psychiatric hospital care-givers.
LIMITATIONS
Aside from the usual limitations of non-randomized non-experimental survey-based research, two additional limitation of the study exist. The first is that the Cronbach alpha coefficients for each of the scales, except the RS-14, were below those reported in previous literature by a range from 0.03 to 0.14 (deviation).This factor could have affected the reliability of the data and consequently the validity of the results. However, the scales with the greatest deviation from published literature were the CCPAI and CS, which were not the main factors related to the research question. Of note, the observed RS-14 Cronbach alpha is within the range of published alphas for this scale and the alphas for PCL-c and STS deviated by 0.09 and 0.05, respectively.
The second issue is that among the measures of TEs, episodes of secondary traumatic events were not collected and analyzed. An observation within this study was that STS appears to be as important as PTSS with respect to BO. Future studies measuring traumatic events should consider measuring episodes of secondary traumatic events as well as primary traumatic events.
Implications for Research, Education and Practice
PTSS and burnout are presumably inter-related, but the findings of this study and the published literature are, overall, equivocal with respect to resilience as a mediating factor. Further exploration of the causes of burnout in the population of psychiatric hospital care-givers is needed to understand the mechanisms and to identify methods to reduce the development of burnout. This exploration might focus on specific stress management and trauma-processing coping skills that can be taught, learned, practiced and employed in the workplace and in care-givers’ non-work experiences. In addition, a focus on compassion satisfaction and its relationship to resilience and burnout might be further explored.
In summary, this study observed that episodes of trauma, stress resilience and compassion satisfaction, combined, robustly predict burnout (explained variance=65%), but that each variable is a weak predictor. In addition, resilience was not related to trauma and stress and did not mediate burnout. This finding presents a paradigm suggesting that there may be two distinctly separate pathways affecting burnout. The literature is limited and does not serve to validate these findings. For care-givers working in highly stressful or trauma-experiencing environments, the findings of this study suggest that resilience may play a minimal role in the avoidance of burnout in relation to stressful and traumatic experiences and may be more important with respect to role satisfaction.


