INTRODUCTION
The United States resettles more refugees than any other nation, accepting between 40,000 and 80,000 annually.1 Frequently coming from dangerous, unsanitary conditions without consistent access to health care resources, these populations often arrives in desperate need of quality health care.2-6 Additionally, unlike many receiving nations, the United States prioritizes the admission of refugees with significant health concerns, further creating populations with pervasive and unique health care needs.5,6,7 While all refugees face significant barriers in resettlement, there is evidence to suggest that women may be particularly burdened by forced migration.2 According to a 2008 report by the United Nations High Commissioner for Refugees, the outbreak of conflict and subsequent displacement exacerbates already existing gender inequalities, resulting in a disproportionate strain on women’s health.8
To address the health concerns of this vulnerable population and to ease transition into the American health care system, refugees are granted the same health care rights afforded to United States citizens and receive a brief period of public health insurance. However, research shows that despite such provisions, refugee women face significant barriers in understanding and accessing appropriate care for themselves and their families. Common barriers identified in recent studies include language barriers, difficulty finding the appropriate provider for specific needs, lack of awareness about health care services and their functions, financial restraints, concerns about confidentiality, the stigma of being diagnosed with certain diseases, and a lack of culturally competent care, including appropriateness of interpreters.3,5,9,10,11
Of particular concern is the inability of many refugee women to overcome the geographic barrier of accessing healthcare. As noted by Garfield, women view their geography in terms of landmarks and rely more on 3-D visualizations, such as buildings and/or natural structures.12 Lack of familiarity with navigating by map and having access to only 2-D maps may hinder women’s ability to identify methods for using the resources (e.g., transportation stops, clinics, major roads, etc.) they need for themselves and their families. Given that most maps are 2-D, with limited incorporation of 3-D structures, it is unclear how refugee women are able to incorporate their preferred geospatial understanding into a new environment. In a study of Cambodian refugees, researchers found that over 50% reported they were sometimes or always unable to see a doctor due to lack of transportation.13 Similar findings have been reported by researchers working with a variety of refugee populations.3,14,15 However, there is evidence to suggest that access to transportation is not the only geographic barrier refugees face in accessing care. Research has found that individual perception about the size of one’s neighbourhood or “own” territory is often correlated with socio-demographic characteristics.16,17,18 In particular, recent migration and low income, characteristics of most refugees, are correlated with the perception of one’s neighbourhood as a particularly small geographic area.17 There is also evidence to suggest that refugees may not feel comfortable leaving the boundaries of their familiar neighbourhoods, even when transportation options are available. For example, one study found that despite affordable and convenient public transportation, many refugees did not feel confident in their ability to use these resources and would rather miss their medical appointment than try to navigate the linguistic and cultural challenges of unfamiliar territory.18
Together, these studies suggest that refugees may have a limited geographic area they consider to be “their” territory and that navigating outside those boundaries may be particularly difficult. Although it is clear that transportation is a central barrier to accessing healthcare, further research is needed to understand refugees’ perception of their neighbourhood and to assess their mobility both within and outside of these boundaries.
In spring 2014, the Refugee Reproductive Health (RRH) Committee hosted a workshop for Congolese women refugees. The purpose of the workshop was to explore how the community defined “health” in the broadest possible sense.19 The RRH Committee had been working together for over two years with various refugee communities to provide workshops on topics of interest to these groups. The RRH Committee is composed of individuals from state government, refugee communities, and university. We spent three months planning the workshop topic and inviting presenters, as well as obtaining incentives for workshop participants. Members of the RRH Committee, including Congolese female community leaders, volunteered to transport participants from their homes or other locations so that they could participate in the workshop. The majority of refugee women from the Congolese community do not drive; therefore, transportation to/from events is always an issue. We discussed having the workshop participants take public transportation, but decided that in order to have individuals arrive in a timely manner we should provide transportation for these women. As volunteers set out to pick up the workshop participants, a number of problems arose. We identified three specific issues:
• We had thought that other members of the Congolese community could transport female participants; however, the female community leaders stated there were a number of cultural issues that prohibited that from happening;
• We had one set of volunteers picking up the participants for the workshop and a second set of volunteers taking people home after the workshop; and
• Volunteers, community leaders, and/or RRH Committee members had not communicated well enough about transportation needs and expectations, and refugee women were not familiar enough with their “new” communities to navigate their own neighbourhoods effectively.
Once the workshop was completed, the RRH Committee met to discuss the various issues that impacted workshop implementation.
First, the cultural parameters for having non-family members provide transportation for workshop participants was a large problem. A number of women from the community mentioned that cultural expectations about “sexual favors” between men and women made them very uncomfortable. So having male community members (who might be more familiar with neighbourhood landmarks, etc.) volunteer to provide transportation was not a workable solution.
Second, it was unclear to volunteer drivers where the refugee women lived. Community leaders had no address or phone list available so that it would be easy to determine where to collect the participants.
Third, there was no clear sense for the workshop participants that volunteers would be picking them up at a specific time and/or place for the afternoon workshop. As a consequence, volunteers drove around the city, locating participants and then made a number of trips back and forth so that participants not yet in attendance, but identified by attendees as they arrived, could attend the workshop.
Fourth, once the workshop was completed, participants could not tell the new set of volunteer drivers what their addresses were nor how to get back to their residences. Volunteers drove around attempting to locate familiar landmarks with the participants, which was very problematic because participants could not provide an idea of what was a familiar landmark.
The stress felt by all surrounding the workshop transportation issues led us to consider what could be done to ensure that these needs and expectations could be addressed more concretely for the next set of workshops for refugee women. Although having a listing of residence locations of refugee groups would have been helpful, we also needed a better understanding of where refugee women lived, what were the resources in their communities, and how refugee women viewed their neighbourhoods and community boundaries?
For this article, we identified critical resources that women from the refugee communities might have in their neighbourhoods. The purpose of the article is to describe our process in identifying these resources so that we can move to the next step of working with women in the communities to determine how they view their neighbourhoods and the resources therein.
METHODS
ArcGIS (version 10.2. Redlands CA: Environmental Systems Research Institute) mapping software was used to map the spatial distribution of refugee residences and basic resources across Salt Lake County. The Refugee Resources Manual provided addresses for seven apartment communities with significant resettled refugee populations.20 Five additional apartment communities with refugee residents were identified by personnel from the refugee resettlement agencies and the Utah Department of Health. The addresses for these refugee residences were geocoded in ArcGIS, a process by which elements are assigned spatial coordinates based on street address, city, and zip code.
Shape files for roads, healthcare facilities, libraries, bus routes, and light rail routes were obtained from the Utah Automated Geographic Reference Center (http://gis.utah.gov/data/). These shape files were uploaded directly into ArcGIS with slight modification. The healthcare facilities shape file included addresses for a broad variety of health-related resources that were deemed not relevant to this particular study (e.g., nursing homes, hospice centers, etc.). Authors RJ and LHG reviewed the list and limited the addresses to hospitals, emergency rooms, urgent care facilities and clinics where primary care services were offered. The bus route shape file was modified to exclude all inter-county express routes, as these were also deemed irrelevant to the current study. The shape file for libraries was modified to include public-access libraries only. Public libraries were included because they offer information on healthcare resources in Salt Lake County and serve as an important source for internet access for many refugees.
Addresses for grocery stores for six major chains located in the Salt Lake County area were identified from the respective corporate websites (www.dansfoods.com, www.freshmarketstores.com, www.harmonsgrocery.com, www.reamsfoods. com, www.smithsfoodanddrug.com, www.walmart.com). Halal markets, an important source of certain food items for Muslim refugees, were identified by a member of the Somali refugee community. The addresses for grocery stores and halal markets were geocoded in ArcGIS.
All shape files and geocoded addresses were combined to simultaneously map refugee residences, transportation routes, and resources. Distances from each residence to the nearest healthcare facility, library, grocery store, and halal market were measured in Arc Map as the shortest distance by road. Estimated travel times from each residence to the nearest resource of each type were calculated using the public transportation feature of Google Maps. The address of the residence and location of the resource were entered and the shortest travel time between 12:00 p.m. and 1:00 p.m. on a standard weekday was recorded.
One-way distance and travel time from residences to resources were graphed as box-and-whiskers plots using Stata (version 13.1, College Station, TX). The box represents the middle 50% of data points (either distance or travel time); the ends of the box correspond to the 25th and 75th percentiles and the line embedded in the box corresponds to the median. The ends of the whiskers generally represent the minimum and maximum observations. In cases where there are outliers in the data, the whisker represents the data point that does not exceed 1.5 times the box width and the outlier data points are marked with a dot beyond the whisker.
DISCUSSION
Based on these mapping data and resource elements, it is clear to us that spatial location presents barriers to the establishment of a refugee support network. Refugee housing is dispersed across a large geographic area (approximately 42 square miles) with substantial internal boundaries (e.g., Interstate 15 or I-15). A point of interest is that refugee groups are not housed by community of origin. Members of one community could be housed up to 13 miles apart. In addition, many refugees do not speak English well enough to establish networks within their residential community with individuals or groups outside their community of origin. Many refugees reside in “resource deserts.” Four of the 12 residences had no resources within one mile. All of these issues lead to a very isolated existence in the Salt Lake Valley, and hinder attempts to gather community members for profession- and/or community-centered meetings.
Figure 1 illustrates the resources that are available near the refugee women’s residences (n=12). The following are clearly indicated on this map:
Figure 1: Location of refugee residences and health-related resources.
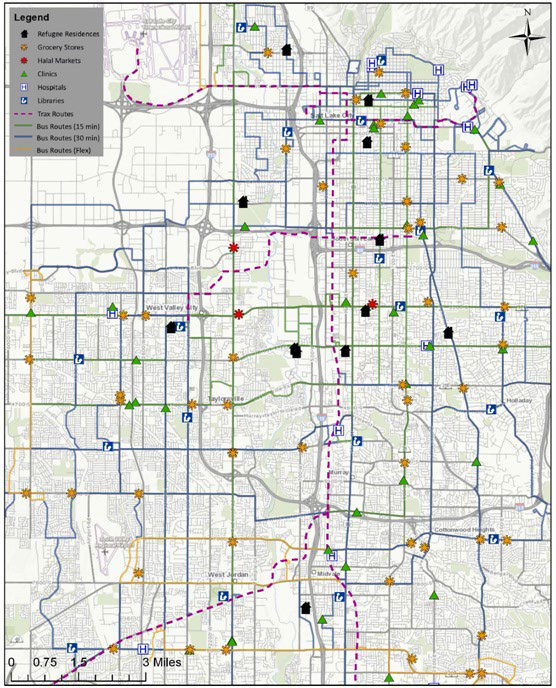
Most residences are on or near a public transportation route only one residence was not
• Five of the residences were near a public library resource
• Eight of the residences were near a clinic
• Two residences were near a hospital-in fact these two residen ces were near six hospitals of varying types
• Seven residences were near grocery stores; one was also near a halal market
• Three residences were near one another—although one residence was on the other side of I-15 (a major freeway)
As highlighted in Figure 2, the median distances from residence to resource suggest resources are often too far away to regularly reach by walking:
Figure 2: Distance to resources (one-way, in miles).
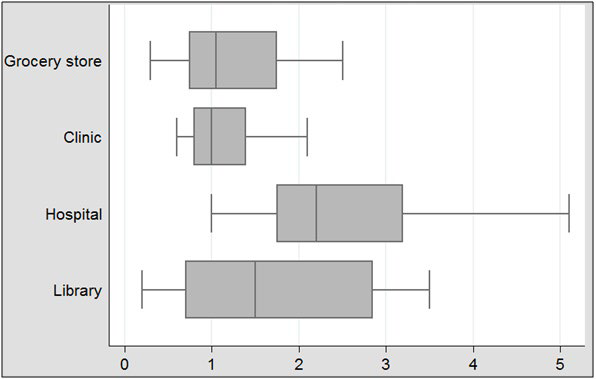
Grocery store: 1.05 miles
Halal market: 2.90 miles
Clinic: 1.00 miles
Hospital: 2.20 miles
Library: 1.50 miles
Since the majority of refugee women do not own a car of their own and do not drive, these women must rely on community members and/or public transportation when they need to access resources in their communities. However, as shown in Figure 3, using public transportation can take considerable time.
Figure 3: Public transportation travel times (one-way, in minutes)
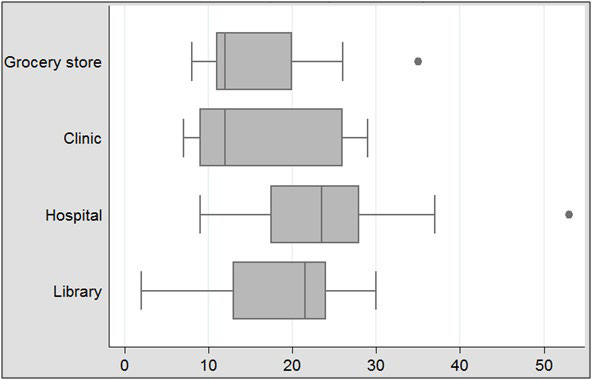
Figures 2 and 3 should be considered within the context of other factors that may impact traveling to and from needed resources for refugee women. First, the duration of the time for traveling to and from resources were taken from the 12:00 p.m. hour on a week day. Early mornings and evenings may be more problematic because of higher traffic rates and increased numbers of travelers. In some cases, people may have to wait for a second train or bus before they can reach their destination. Along with the time issue, travelers will need to navigate the process of transferring to other routes to reach their destinations.
Second, Utah has winter weather where snow can halt a bus service and/or make public transportation run late. Thus, women need to travel in inclement weather, which may not be temperatures they are accustomed to if they have come from a more moderate or tropical climate. If a woman needs to travel in the snow and make a number of transfers to reach her location, she may decide not to travel at all and go without what she needs from the resource.
Third, public transportation in Utah runs more frequently and consistently during week days and daylight hours. If she has a job that is early in the morning, late in the evening, a graveyard shift, and/or a weekend shift, the woman may not be able to access public transportation to get to her job. Buses on the weekends, especially Sundays, run every 60 to 90 minutes beginning at 12:00 pm. until about 6:00 pm. on certain routes. Not all routes are available on weekends.
CONCLUSIONS
This descriptive article explores the impact of resource locations, geospatial settings, and public transportation on refugee women’s ability to access these services. It is clear from the geospatial discussion that refugee women are unclear about how to identify the landmarks in their neighbourhoods and how those landmarks connect to resources. In fact, some refugee women live in resource deserts and need to travel significant distances to obtain the resources they need.
The next steps for our work will be to establish perceived neighbourhood boundaries and navigation techniques among refugees of various communities of origin. We plan to utilize GoPro cameras to walk with refugee women as they navigate their neighbourhoods, travel to and from their jobs, and access health and other community resources. With these activities, we can determine the needs of refugee women in this arena. This information will be transferable in discussing resettlement issues for various refugee groups.
In addition, we will examine the differences in how refugee women and men navigate to resources across this Intermountain West city. We plan to obtain information from refugee groups about how they understand and “see” their neighbourhoods and communities as well as the resources in these communities. Once we have a better understanding of these issues, we will work with providers and refugee women to develop a more comprehensive discussion about how to navigate to resources and how to obtain needed services.
IMPLICATIONS FOR HEALTH CARE PROVIDERS
In making treatment or referral recommendations for refugees, providers and clinical staff may need to consider geospatial issues. For example, is there a pharmacy in the neighbourhood setting where a prescription can easily be filled or will this patient have to travel outside his/her own neighbourhood to obtain the prescription? If the latter, then identifying contiguous neighbourhoods that can reasonably be accessed and/or identifying appropriate public transportation routes to a pharmacy could be important in empowering a refugee to adhere to a clinical recommendation.
In addition, providers should develop a sense of what resources are available for refugee communities given their addresses. Directions to resources should be provided in terms of landmarks with which clients would be familiar rather than street name or cardinal directions.
The overall take away message is that providers in all health and allied health fields need to be more aware of the types of resources and their locations so that information can be adequately provided for refugee client populations.


