INTRODUCTION
Successful management of dental caries in pediatric patients is considered a difficult task given to the challenges, including access to care, behavior management and the need for sufficient effective treatment until tooth exfoliation.1 Aesthetics is a branch of philosophy dealing with beauty and the beautiful. The term cosmetic dentistry can be used to describe dental procedures for improving the patient’s appearance even in the absence of pathology. Dental aesthetics, on the other hand, refers to the skills and techniques used to improve the form and symmetry of the teeth and face in order to improve both the appearance and function of the teeth, mouth and face. Therefore, pediatric aesthetic dentistry is “a branch that deals with the maintenance and enhancement of the beauty of the mouth of infants and children through adolescence, including those with special healthcare needs”.2 Kapur et al3 in 2005 reported that aesthetic rehabilitation of the primary dentition has psychological benefits as well as functional benefits.
Proper treatment of carious primary teeth plays a major role in preventing oral infections, maintaining proper mastication and space in the arch for the permanent teeth. The Hall technique is a conservative alternative treatment for carious primary molars developed by Dr. Norna Hall in the 1980s. This technique involves “the use of stainless steel crowns to seal over caries lesions on primary molars by using glass ionomer cement”; it is performed without caries removal, neither crown preparation nor administration of local anesthetic.4
In a randomized controlled clinical trial, investigators found that stainless steel crowns placed using the Hall technique outperformed standard Class II restorations placed by general dentists.5 In addition to achieving comparative restoration success, the Hall technique was preferred over traditional restorative techniques by children, caregivers and dentists.6
The aim of the present study was to evaluate the effectiveness of acrylic crown in restoring carious maxillary primary incisors following the Hall technique. Clinical follow-ups were carried out on a 3, 6 and 12 monthly basis.
MATERIALS AND METHODS
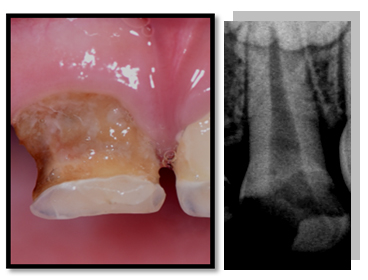
Ten healthy children aged 2-4 years of both genders, with extensive carious maxillary incisors were involved in this study (Figure 1). The study was extended from October 2015 to May 2017. After a complete clinical and radiographical examination for carious incisors, detailed treatment plans were explained to the children’s parents and written consents were obtained for including the children in this study. Instructions on oral hygiene and crown maintenance were given to the parents.
Figure 1: Pre-Operative Clinical and Radiographical Views Showed Extensive Carious Maxillary Primary Incisor.
The Excluded Criteria were as Follows5
• Clinical signs or symptoms of irreversible pulpitis, or dental abscess;
• Radiographic signs or symptoms of dental abscess or pulpal involvement;
• Phathological mobility.
Construction of Fixed Aesthetic Acrylic Bridge
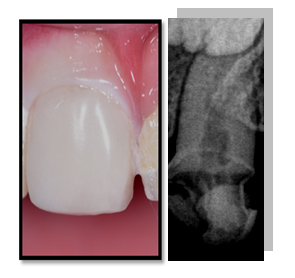
Pre-operative occlusal analysis was performed and impressions for maxillary arch were taken using elastomeric impression material (ORMAMAX, Italy). Working casts were then prepared and the shade/color of the teeth were determined. The working cast was 3D scanned using Activity 710 3D scanner (smart optics Sensortechnik GmbH, Germany). The crowns were designed using the Exocad Program (smart optics Sensortechnik GmbH, Germany). Acrylic block poly-methyl methacrylate (PMAA) was performed on the acrylic crowns using computeraided design and computer-aided manufacturing (CAD/CAM) machine (charlydental, Z.I. Fonlabour, France). After trimming, finishing and polishing the acrylic crowns, the teeth were isolated and dried using an air syringe without giving local anesthesia, without caries removal and tooth preparation. The acrylic crowns were then cemented using Riva Luting glass ionomer cement (Riva, SDI, England) and occlusion was checked for any premature contact (Figure 2).
Figure 2: Post-Operative Clinical and Radiographical Views Showed Aesthetic Acrylic Crown Cemented on Maxillary Primary Incisor. Acrylic Crown is Radiolucent and Glass Ionomer Cement is RadioOpaque.
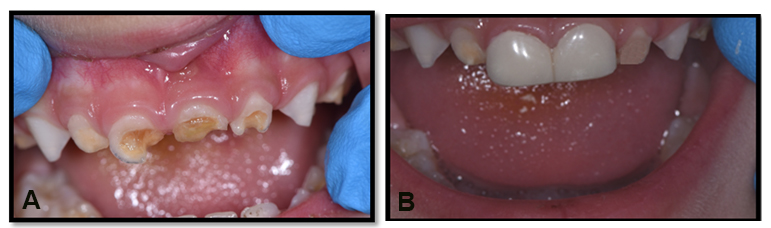
The parents were advised against giving any hard food to the children to avoid chewing and to maintain proper oral hygiene. The data included in this study was obtained from 3, 6 and 12 months follow-up visits (Figure 3). The parents were satisfied with the results of the procedure. Patients were also advised to consult immediately in case of any problem with the crown, including distortion, breakage or any pathological signs and symptoms.
Figure 3: (A) Pre-Operative Image Demonstrate Extensive Carious Maxillary Primary Central Incisors. (B) At 12 Months Follow-Up Visit the Acrylic Crowns were Fit Aesthetically and were Functional.
During the follow-up study, signs and symptoms of clinical and pathological tooth changes (pain, tenderness, periapical pathology, and mobility) were examined if any previous pathology was observed. Radiographical examination was also indicated. Fracture of the acrylic crown (0=no fracture, 1=small fracture, 2=bulk fracture), retention (1=good, 2=fair, 3=poor) and the condition of gingiva were examined. A gingival score on a scale of 0 to 3 was determined: 0=no inflammation; 1=mild inflammation; 2=moderate inflammation; 3=marked inflammation.7
Each child’s parent was asked to provide a feedback for evaluating their satisfaction with the restorations. Criteria used included, (1) appearance; (2) color match; (3) durability; (4) ability to eat and (5) feasibility of teeth brushing. Each of these criteria was scored using the following scale: 1=very dissatisfied; 2=dissatisfied; 3=neutral satisfied; 4=satisfied; 5=very satisfied.8
The data were summarized and described using relative frequencies and percentages for categorical variables. For the resultant categorical variables, t-test was used to compare between means for statistical significance. Data was analyzed using the SPSS software, version 16.0 (SPSS Inc., Chicago, IL, USA) for Windows. Statistical significance was set at p≤0.05.
RESULTS
Figure 4 demonstrates the clinical parameters recorded at 3, 6 and 12 months follow-up visits. Concerning the presence or absence of any signs and symptoms of the pathological changes of the teeth, or fracture of the crown, no fractures were recorded in any of the cases at any recall visits.
Figure 4: Clinical Parameters Recorded at 3, 6 and 12 Months Recall Visits.
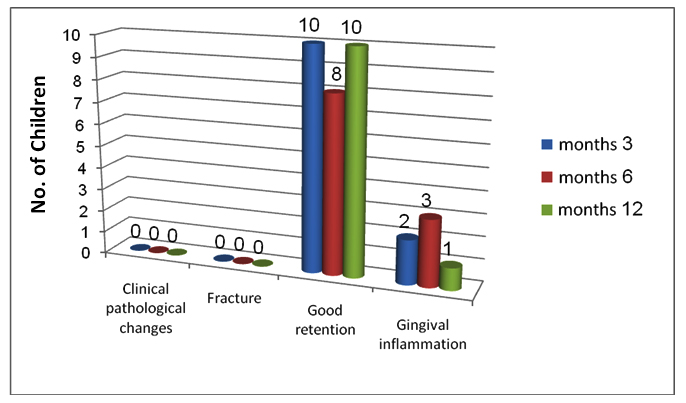
Good retention of the crowns was observed in 100% (N=10) of the cases at 3rd and 12th month visits, whereas only 10% (N=1) of the cases showed poor retention at the 6th month visit, that needed re-cementing.
The gingiva around the crown was inflamed in 20% (N=2), 30% (N=3) and 10% (N=1) of the cases at 3, 6 and 12 months respectively. All of the gingival inflammations were of moderate type.
Table 1 shows the data from the parental satisfaction survey. When comparing between the parental satisfaction at different time intervals for appearance, color match, durability, ability to eat and feasibility of teeth brushing, the means of parental satisfaction were observed to have significantly (p≤0.05) increased with the progression of time.
| Table 1: Parents’ Satisfaction at 3, 6 and 12 Months Recall Visits |
| Parameters |
At 3 months visit (Mean±SD) |
At 6 months visit (Mean±SD) |
At 12 months visit (Mean±SD) |
t-test |
p-value |
| Appearance |
2.7±0.1
|
3.8±0.1
|
4.7±0.1
|
3.08
|
0.00*
|
| Color match |
2.9±0.1
|
3.6±0.2
|
4.6±0.2
|
4.34
|
0.00* |
| Durability |
3.3±0.3
|
4.8±0.1
|
3.3±0.1
|
7.29
|
0.00* |
| Ability to eat |
1.7±0.1
|
3.0 ±0.2
|
4.7±0.1
|
7.05
|
0.00* |
| Feasibility of teeth brushing |
2.7±0.1
|
3.6±0.2
|
4.7±0.1
|
4.27
|
0.00*
|
| *Significant difference at p≤0.05. |
DISCUSSION
Caries management for children differs from that of adults. For adults, the management of an active dentinal lesion is usually straightforward. For children, freedom from pain and infection is their priority, unless which they do not see any problem to be managed.
Recently, biologically-orientated strategies for managing dental caries have come back into focus. A number of clinical trials have been carried out looking at partial, or no caries removal in primary teeth and how the outcomes for these techniques contrast to complete caries removal. These ‘minimal intervention’ approaches reduce some of the adverse consequences associated with carrying out restorative treatment, with the advantages of conservation of tooth structure and integrity, maintenance of maximum pulpal floor dentinal thickness and reduced pulp exposure.
This is the first known clinical study reporting the clinical longevity of using fixed aesthetic acrylic crowns for restoring carious maxillary primary incisors using the Hall technique with a clinical follow-up that extend up to 12 months. Sample size is one of the limitations of this study which is understandable due to the cost of the treatment. Moreover, aesthetic dental treatment in Iraq is not subsidized by the Iraqi Health System, making it a burden for the patients.
In this study, all the crowned primary incisors remain aesthetically and clinically fit without and pathological changes.
Concerning the retention, compatibility and quality of the CAD/CAM acrylic crowns used, the results failed to record any fractures owing to the high modality technique used to prepare the acrylic crowns as well as the type of material used; PMMA, a strong, tough, and lightweight material.9
Concerning retention of the crowns, only 2 of 10 cases showed poor retention during the 6 months follow-up because of the child’s habit of eating sticky food. This was resolved by effectively cleaning the crowns and re-cementing them. The high retention of crowns recorded in this study is due to the chemical bonding properties of Riva Luting glass ionomer cement used in cementation, which chemically bonds to metal substrates and the tooth. High flexural strength enhances longevity of a glass ionomer luting cement by withstanding mastication forces. Riva Luting’s high flexural strength increases its durability in the oral environment and long-term ability to retain indirect restorations. Also, Riva Luting has low solubility in the oral environment. This increases the material’s ability to resist disintegration and wear caused by oral acidity.10
The gingiva around the crown was observed to be inflamed in 2, 3 and 1 out of 10 cases at 3, 6 and 12 months respectively. All of the gingival inflammations were of moderate type because of improper oral hygiene measures. The parents were instructed to follow good oral hygiene measures to control gingival inflammation and prevent progression to severe periodontal problems.
The means of parental satisfaction were significantly (p≤0.05) increased with the progression of time. The primary reason for parents’ satisfaction was the non-use of anesthesia or any caries removal, in addition to the aesthetic appearance, stability of color, durability of the crown, ability of the child to eat normally and feasibility of teeth brushing.
With the Hall Technique, the process of fitting the crown is quick and non-invasive. The crown is seated over the tooth with no caries removal or tooth preparation of any kind, and local anesthesia is not required.
This is the first published study considered to be the modification of the Hall technique for aesthetic restoring of carious maxillary primary incisors. But, the question remains whether the caries lesions restored according to this technique will be sealed successfully and remains arrested until the tooth exfoliates naturally? Gilchrist et al in 2013 published a systematic review showing that in case of incomplete caries, sealing them results in clinical and radiographic signs of inactivation of the caries lesion with tertiary dentin formation.11
Bell et al12 reported a success rate of 93% after 4 years of follow-up and Al-Yaseen et al13 reported 96% over three years of using glass ionomer cement placed directly over carious dentin during indirect pulp therapy in primary teeth.
CONCLUSION
In the present study, the simple technique of aesthetically restoring the carious primary maxillary incisors allows it to be used in daily clinical practice with great success, both to the child and parent in establishing a positive attitude and satisfaction in relation to aesthetics and function of primary anterior teeth.


