BACKGROUND
It is recommended that adults perform at least 2.5-hours of moderate-intensity aerobic exercise or 1.25-hours of vigorous intensity activity or some combination of both types of exercise in a week.1 However, on average, less than five percent of adults participate in 30-minutes of physical activity per day.2 Current evidence suggests that sedentary lifestyles are associated with comorbidities such as obesity, diabetes mellitus and cardiovascular disease,3 as well as poor health outcomes such as hypertension, hyper lipidemia, stroke, metabolic syndrome, osteoporosis, and certain types of cancers.4,5 Though the cause of these comorbidities are multifactorial, a key component to development of these chronic diseases is lack of physical activity. Conversely, increased physical exercise is correlated with a decreased risk for developing these diseases.6
Change is needed. Decades of research into human behavior has expanded our understanding of motivation which is key to any behavior change. Attempts to apply the transtheoretical model and stages of change theory (TTM-SOC) to physical activity, have resulted in non-conclusive findings to support or negate this application of the model.7,8
Transtheoretical Model Defined
The TTM-SOC, was created as a compilation of psychological theories to explain behavior change as related to addiction (Prochaska et al). The TTM-SOC initially included the components of stages of change (SOC), decisional balance and processes of change (POC) with self-efficacy (SE) subsequently added. As a motivational theory used to guide interventions for change, the transtheoretical model (TTM) describes the SOC as progressions a person must advance through for the purpose of making an effective behavior change. The SOC consist of precontemplation, contemplation, preparation, action, maintenance and for some behaviors, termination.9 The TTM purports that each stage aligns with the constructs of decisional balance-the weighing of pros and cons for behavior change; self-efficacy-confidence to make and maintain the change; and processes of change-both cognitive and behavior.9
Previous Research
The TTM has been applied with smoking cessation with physicians and other practitioners adopting stage assessment tools and stage matched interventions.10 Use of the theory has expanded to explain behavior change with regard to exercise and sedentary lifestyles. In a systematic review, authors concluded that there was cautious support for stage matched exercise interventions.11
In a systematic review by Bulley et al,7 (preferred reporting items for systematic reviews and meta-analyses (PRISMA) score=10/27), authors concluded that the accuracy of self-assignment for stages of action or maintenance for physical activity was frequently inconsistent with recommended physical activity guidelines. Furthermore, measurements to assess stages of change for exercise were not found to be valid or standardized, suggesting that more research was needed to investigate the validity of this measure.7,12
Validity limitations of the evidence available for the TTMSOC prior to 2007 include that stage allocation for exercise was linked with self-reported activity, and the physiological parameters (body composition, physical fitness) used are indirect measurements for changes in stage.7 Additionally, though not direct measures of exercise or physical activity, body mass index, weight and girth measurements were used to assess stage progression. With regard to outcome measures used and construct validity, future investigations require validation of instruments with more rigorous methods.7,8 The evidence available regarding TTM-based behavior change interventions applied to exercise as moderate physical activity has been focused upon one component, namely, the stages of change, versus all four of the components of the model.7 An additional recommendation is that the full model should be assessed fully/holistically.8
There is a need to assess whether evidence during the most recent decade has provided more rigorous evaluation and application of the TTM-SOC with and its full components with regard to physical activity.
PURPOSE
The purpose of this review was to determine how the TTMSOC has been applied for adoption of physical activity in the last 10-years.
METHODS
Search Strategy
The following databases were searched and accessed May 2017 with updates January 2018 and May 2019: PSYC Info, ERIC, CINAHL, EBM, DARE, OVID. Key search terms for this literature review included: “Lifestyle Changes” OR “Lifestyle” OR “Active Living” OR “Lifestyle Changes” OR “Physical Activity” OR “Actigraphy” OR “Exercise” OR “Activity Level” AND “Transtheoretical Model” OR “Stages of Change.” Inclusion criteria consisted of full text availability, English language, peer reviewed investigations published in the last 10-years, relating to Transtheoretical Model Stages of Change and its application to influence health outcomes via physical activity were included in the study. Searching the following additional databases, namely, American Periodicals, ART bibliographies Modern (ABM), British Periodicals, Digital National Security Archive, ebrary, e-books, GeoRef, PAIS Index, Periodicals Archive Online, ProQuest Dissertations & Theses Global, SciTech Premium Collection, nine (9) articles were found. Of these, all non-peer reviewed findings were omitted.
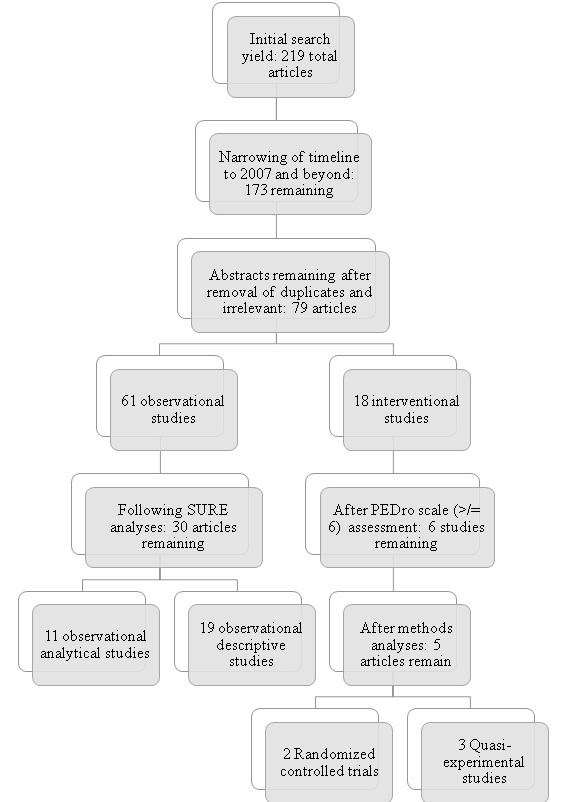
Inclusion criteria: Investigations that were 1) related to the use of the TTM with physical activity, 2) performed with adults, 3) peer-reviewed, 4) published after 2007, and 5) in the english language (Figure 1).
Figure 1. Investigations Assessment Flowchart
Initial Review
The search dating 2007-2019 yielded 126 articles. Investigations of reliability and/or validity of model constructs were sequestered from experimental design/randomized controlled trials, though all were organized for further review. Following removal of excluded articles and all subsequent duplicates from overlapping databases, a total of seventy-nine (79) relevant articles were assessed for rigor and inclusion (Figure 1). Articles were organized into two categories: 1) observational (n=61), which included descriptive or analytical studies,and 2) interventional (n=18), consisting of randomized controlled and quasi-experimental studies (Table 1).
| Table 1. Summary of Interventional Studies |
|
Author/Year (Design)
|
Purpose |
Study Limitations
|
Population |
|
Findorff et al15 (RCT)
|
To determine whether cross-sectional and longitudinal patterns of exercise adoption reported by older women participating in a randomized trial of an exercise-based fall reduction program would conform to the TTM. |
Stage of Change was only variable assessed in control group
|
Female older adults |
|
Jackson et al17 (RCT)
|
To determine behavior change for physical activity in people with type 2 diabetes in differing stages of change, as a result of delivery of TTM exercise intervention. |
Does not measure 3 of 4 constructs of TTM*
|
Adults with Type 2 Diabetes |
|
Fischer et al16 (Quasi-experimental)
|
To determine effectiveness of certified personal trainer services in promoting exercise adherence in female traditional-aged college students
|
Stage specific approach not used
|
Female, traditional-aged college students |
|
Prochaska et al18 (Quasi-experimental)
|
Comparison of initial efficacy of motivational interviewing, online TTM-tailored communications, and brief Health Risk Intervention on 4 health risk factors: inactivity, BMI, stress, smoking |
Combined with other theoretical models (Health Risk Intervention, Motivational Interviewing); poor recruitment (25%) and retention (70%) rates; does not measure 4 of 4 constructs of TTM
|
Adult, university employees |
|
Yang et al19 (Quasi-experimental)
|
Application of TTM to test effects of senior elastic band (SEB) exercises on functional fitness in older adults in contemplation, preparation stages of behavioral change |
Does not measure 3 of 4 constructs of TTM; significant differences between groups in lower body flexibility at baseline; convenience sampling
|
Community older adults (65yrs+), who can stand independently with no AD |
Measurement Instruments
Investigators applied the PEDro scale13 to interventional investigations. Inclusion or exclusion was not based upon PEDro scores exclusively, rather, investigations scored >6 were reviewed for validity of methodology and if strong, were included. Investigations with PEDro scores <5 were excluded.
The Specialist Unit for Review Evidence14 checklist, specific to cohort or cross-sectional, non-experimental design investigations was chosen to assess the non-interventional investigations (Figure 2) using recommendations regarding critical appraisal checklists.15
| Figure 2. Cardiff University: SURE Checklist |
|
Questions to Assist with the Critical Appraisal of Cohort Studies
|
| For all questions below, “yes/no/can’t tell”
1. Is the study design clearly stated?
2. Does the study address a clearly focused question? Consider: population; exposure (defined and accurately measured); Comparator/control; outcomes
3. Are the setting, locations, and relevant dates provided? Consider: recruitment period; exposure; follow-up & data collection
4. Were the participants fairly selected? Consider: eligibility criteria; sources & selection of participants; method of follow-up; for matched studies – details of matching
criteria and number of exposed or unexposed
5. Are participant characteristics provided? Consider if: sufficient details; a baseline table is included
6. Are the measures of exposures & outcomes appropriate? Consider if the methods of assessment are valid and reliable.
7. Was bias considered? E.g. recall or selection bias
8. Is there a description of how the study size was arrived at?
9. Are the statistical methods well described? Consider: how missing data was handled; were potential sources of bias (confounding factors) controlled for; how loss to
follow-up was addressed
a. Consider threats to internal validity (all 8, including): _____
10. Is information provided on participant flow? Consider if following provided: flow diagram; numbers of participants at each stage; details of drop-outs; details of missing
participant data; follow-up time summarized; numbers of outcome events
11. Are the results well described? Consider if: effect sizes, confidence intervals/standard deviations provided; the conclusions are the same in the abstract and full text
12. Is any sponsorship/conflict of interest reported?
13. Finally…did the authors identify any limitations and, if so, are they captured above? |
| *Specialist Unit for Review Evidence (SURE)14 |
RESULTS
Systematic Reviews
No systematic reviews regarding the TTM-SOC and exercise behavior change were found for the past ten years. This lack of synthesis of recent evidence further validates the need for the current systematic review.
Interventional Studies
Of the eighteen (18) interventional studies meeting the inclusion criteria, six (6) scored > 6/11 on the PEDro Scale, so judged ‘moderate quality.’ Further in-depth analysis of methodology deemed five (5) to be of moderate to high quality evidence and retained. Of these five (5) investigations, three (3) were quasi-experimental and two (2) were randomized controlled trials.16-20 Of these five (5) articles, two (2) clearly assessed all four constructs of the Transtheoretical Model: self-efficacy, decisional balance, stages of change, and processes of change.16,17
Limitations of the intervention studies included that there was a lack of true stage-matching and there was a failure to account for individuals in precontemplation and contemplation who did not have any intention to take action towards physical activity (Table 1). Though these investigations purported to test movement through the stages of change, none of these studies provided stage-matched interventions to assess cause-effect, nor tightly controlled the intervention. Therefore, identified investigations maintained common limitations regarding the TTM-SOC noted in prior decades regarding application to physical activity (Tables 2-7).
| Table 2. Summary of Results (Interventional Studies): Stages of Change |
| Stage of Change |
|
Author
|
Finding
|
Results
|
|
Findorff et al15 (RCT)
|
Individuals with TTM intervention demonstrated increased progression through SOC to become exercise adopters
|
p value <0.001 CI, SD, effect size not avail
|
|
Jackson et al17 (RCT)
|
Individuals receiving exercise consultation interviews demonstrated increased success rates of stage progression versus control group with no consultation
|
p value 0.007 CI, SD, effect size not avail
|
|
Fischer et al16 (Quasi-experimental)
|
Within-group comparison of stage of exercise change from T1 to T2 was significant for the control group.
|
p value<0.001, α=0.05 CI, SD, effect size not avail
|
|
Prochaska et al18 (Quasi-experimental)
|
At 6 months, motivational interviewing and TTM-based intervention groups both demonstrated significantly greater proportions of individuals at criteria (exercising moderately 30 minutes/day for at least 5 days/ week) for exercise, as compared to health risk intervention only group.*
|
p value≤0.01 CI, SD, effect size not avail
|
|
Yang et al19 (Quasi-experimental)
|
Participant stages were identified in demographic profiles. Progressions were addressed in article discussion, minimal descriptions.
|
N/A
|
| * Action phase was singularly assessed in the study Prochaska et al.18 at follow-up post-intervention. This indicated a greater number of individuals meeting criterion of the action stage versus individuals who did not meet this stage. |
| Table 3. Summary of Results (Interventional Studies): Decisional Balance |
| Decisional Balance |
|
Author
|
Finding
|
Results
|
|
Findorff et al15 (N=272)
|
No difference among control versus intervention groups
|
p-value>0.05
|
|
Jackson et al17 (N=34)
|
Decisional balance not assessed in this study
|
N/A
|
|
Fischer et al16 (N=62)
|
Significant decrease (negative trend) from T1 to T2 for decisional balance among control group in a measure of which the higher the score, the more beneficial the exercise (pros) is perceived to be.
|
p-value 0.002, Effect size 0.60, CI, SD not avail |
|
No significant decrease (no negative trend) among experimental group with personal training services in a measure of which the higher the score, the more beneficial the exercise (pros) is perceived to be.
|
p-value 0.461 CI, SD not avail
|
|
Prochaska et al18 (N=1400)
|
Decisional balance not assessed in this study |
N/A |
| Yang et al19 (N=169) |
Decisional balance not assessed in this study
|
N/A
|
| Table 4. Summary of Results (Interventional Studies): Processes of Change |
|
Processes of Change
|
|
Author
|
Finding
|
Results
|
|
Findorff et al15 (N=272)
|
Increased use of behavioral processes was demonstrated in exercise adopters between T1 and T2
|
p-value<0.001 |
| Jackson et al17 (N=34) |
Decreased use of cognitive processes was demonstrated in exercise adopters between T1 and T2
|
p-value<0.001
|
|
Fischer et al16 (N=62)
|
Within-group comparison of exercise mediators at T1 and T2 demonstrated significant decrease (negative trend) among control group for cognitive processes
|
p-value 0.016 |
|
Within-group comparison of exercise mediators at T1 and T2 demonstrated significant decrease (negative trend) among control group for behavioral processes
|
N/A
|
|
Statistically significant decrease (negative trend) among experimental group with personal training services for behavioral processes
|
p-value 0.006, t[30]=2.963 Effect size 0.53 CI, SD not avail |
|
No significant decrease (negative trend) for cognitive processes among experimental group with personal training services
|
p-value<0.001, t[30]=4.497 Effect size 0.81 CI, SD not avail
|
|
Prochaska et al18 (N=1400)
|
Processes of change not measured in this study |
N/A |
| Yang et al19 (N=169) |
Processes of change not measured in this study
|
N/A
|
Stages of Change
All five (5) interventional studies reported on the stages of change, four (4) of which utilized some variant of a self-report questionnaire to measure the SOC for exercise.16,17,18,20 One (1) remaining study lacked clarity with assessment of the stages, though the exercise SOC appeared to be assigned by the researcher if the participant met a criterion for exercise.19 Between-stage movement was assessed for exercise SOC among three (3) studies.6,17,18 Where regression was noted, one (1) study offered strategies and discussions to overcome the relapse in stages.16 Data was correlated with its relation to the current SOC in two (2) studies16,18 and in one (1) study, subjects were categorized into their SOC based on a measured amount of physical activity.18
Decisional Balance
Measured in two (2) of the five (5) included studies, decisional balance was assessed for exercise via self-report questionnaire.16,17 In both of these studies, there were longitudinal comparisons of decisional balance scores throughout the study,16,17 and one (1) of these studies correlated decisional balance with a SOC measurement.16
Self-Efficacy
Two (2) studies measured SE, which was assessed via self-report questionnaires.16,17 Longitudinal assessments of SE from baseline to follow-up were included in both of these studies,16,17 and in one (1) of these, decisional balance was compared with SOC at postintervention.16 This study also used data to determine if SE scores at baseline predicted adoption of exercise by post-intervention.16 Additionally, three types of SE for task, coping, and scheduling were measured in one (1) study via a self-report scale.17
| Table 5. Summary of Results (Interventional Studies) |
| Self Efficacy |
|
Author
|
Finding
|
Results
|
| – |
Self-efficacy was significant predictor of whether a person would become an exercise adopter long-term
|
p-value<0.05 CI 1.04-1.14, SD, effect size not avail
|
|
In comparison of T1 to T2 at post-intervention, self-efficacy scores for exercise adopters decreased
|
p-value 0.43
|
|
In comparison of T1 to T2 at post-intervention, self-efficacy scores for exercise readiness group decreased
|
p-value 0.29 SD, CI, effect size not avail
|
|
Jackson et al17 (N=34)
|
Self-efficacy not assessed in this study
|
N/A
|
|
Fischer et al16 (N=62)
|
Within-group comparison of exercise mediators at T1 and T2 demonstrated significant decrease in scheduling self-efficacy for control group |
p-value 0.004, Effect size 0.57, CI, SD not avail |
|
Within-group comparison of exercise mediators at T1 and T2 demonstrated no significant change for task self-efficacy among control group
|
p-value 0.863, Effect size 0.03 CI, SD not avail
|
|
Within-group comparison of exercise mediators at T1 and T2 demonstrated no significant change for coping self efficacy among control group
|
p-value 0.059, Effect size 0.35, CI, SD not avail
|
|
No significant decrease (no negative trend) among experimental group with personal training services for coping self-efficacy, scheduling self efficacy, or task self-efficacy which indicates maintenance or progression in this group.
|
p-value>0.05, CI, SD not avail
|
|
Prochaska et al18 (N=1400)
|
Processes of change not measured in this study |
N/A |
| Yang et al19 (N=169) |
Processes of change not measured in this study |
N/A
|
| Table 6. Summary of Results (Interventional Studies): PA Outcome Measures |
| Outcome Measure of Physical Activity (Objective) |
|
Author
|
Finding
|
Results
|
|
Findorff et al15 (N=272)
|
Walking behavior, as measured by daily exercise logs [primary outcome used for categorization of SOC] demonstrated a significant difference for between-group comparison of individuals in experimental group who became exercise adopters more frequently than the control group.
|
p-value<0.01
|
|
Jackson et al17 (N=34)
|
Among TTM-based intervention, experimental group receiving exercise consultation interviews demonstrated significant change from initial measure in PA levels to 6 weeks |
p-value<0.01 CI, SD, effect size not avail |
|
Among TTM-based intervention, experimental group receiving exercise consultation interviews demonstrated significant change in PA levels after 6 weeks as compared to control group PA levels
|
p-value<0.01 No additional values avai
|
|
Significant difference for experimental group duration of PA as compared to control group
|
p-value<0.05 No additional values avail
|
|
Fischer et al16 (N=62)
|
Experimental group with personal training services demonstrated significantly more positive pattern of exercise behavior as compared to control group (adherence)
|
p-value 0.028, Contingency coefficient=0.358 CI, SD, effect size not avail
|
|
Prochaska et al18 (N=1400)
|
Primary outcome measure to meet criterion for physical activity was stage of change. Objective PA not clearly tracked in this study. |
N/A |
| Yang et al19 (N=169) |
Objective PA not tracked in this study |
N/A
|
| Table 7. Summary of Results (Interventional Studies): Other Outcome Measures |
|
Outcome Measure
|
|
Author
|
Finding
|
Results
|
|
Yang et al19 (N=169)
|
With implementation of senior elastic band program, experimental group participants who engaged in the activity demonstrated significant outperformance at all time points (3- and 6-months) versus control group in: lung capacity, cardiopulmonary fitness, upper and lower body flexibility, upper limb muscle power, and lower limb muscle endurance
|
p-value<0.05 , Effect size 0.2, CI, SD not avail |
|
All 6 variables (lung capacity, cardiopulmonary fitness, upper and lower body flexibility, upper limb muscle power, and lower limb muscle endurance) were significant for experimental group in comparison of pre-test and 6 months later at post-test
|
p-value<0.01 CI, SD, effect size not avail
|
|
Among control group with no elastic band exercises, lung capacity changed significantly from pre-test to post-test at 3- and 6-months
|
p-value 0.34, F=3.61, CI, SD, effect size not avail |
| Among control group with no elastic band exercises, cardiopulmonary fitness changed significantly from pre-test to posttest at 3- and 6-months |
p-value<0.01 F=14.91, CI, SD, effect size not avail
|
| Health Risk Factors |
|
Prochaska et al18 (N=1400)
|
At 6 months, TTM and motivational interviewing groups both had significantly greater percentage of participants reaching criterion for effective stress management compared to health risk intervention group |
p-value<0.01 CI, SD, effect size not avail |
| At 6 months, health risk intervention group demonstrated significantly greater number of health behavior risks than motivational interviewing and TTM groups |
p-value<0.05 CI, SD, effect size not avail
|
| Supplemental Table 8. Summary of Findings (Observational Descriptives of Moderate Quality) |
|
Author/Year (Study)
|
Population/Age/Ethnicity Investigated |
Diagnoses? |
S U R E
Score*
|
|
Dumith et al22
|
Southern Brazil |
N/A |
12/14 |
| Kim23 |
Korean [college students] |
N/A |
10/14
|
|
Rogers et al24
|
Adult females |
Breast cancer |
11/14 |
| Basta et al25 |
Adults |
HIV-positive |
9/14
|
|
Dunton et al26
|
Middle-aged/Community dwelling adults/United States |
N/A |
10/14 |
| Rhodes et al27 |
Employees/Province of Alberta |
N/A |
14/14
|
|
Sørensen et al28
|
Norwegian |
N/A |
9/14 |
| Cardinal et al29 (Cohort) |
University students/South Korea/United States |
N/A |
9/14
|
|
Cengiz et al30 (Cross-sectional survey)
|
University students/Turkey |
N/A |
10/14 |
| Lutz et al31 (Longitudinal) |
Undergraduate students/female/United States |
N/A |
11/14
|
|
Bezyak et al32 (Survey)
|
Adults |
Mental illness (including schizophrenia, schizoaffective disorder, bipolar disorder, other mood disorders, and other psychotic disorders) |
9/14 |
| Jiang et al33 |
American Indian/Alaska Native adults |
Pre-diabetes |
10/14
|
| Kosma et al34 (Longitudinal) |
Adults |
Physical disabilities (including multiple sclerosis, spinal cord injuries) |
|
|
Malone et al35
|
Adults |
Physical disabilities and chronic health conditions (Disabilities or chronic conditions considered to be neuromuscular (such as, cerebral palsy, Parkinson’s disease, spinal cord injury, stroke, traumatic brain injury), orthopedic (such as amputation, arthritis, lw back pain, scoliosis), cardiovascular or pulmonary (such as COPD, dyslipidemia, heart disease, hypertension) and multiple (combination of 2+ disabilities or chronic conditions) |
|
| Yildirim et al36 |
Turkish /Women in low or high SES neighborhoods |
N/A |
11/14
|
|
Johnson et al37
|
Undergraduate students/ Community volunteers/Adults |
N/A |
10/14 |
| Colangelo38 |
Women |
N/A |
12/14
|
|
Duan et al39
|
China/Germany/University Students |
N/A |
11/14 |
| Kaasalainen et al40 |
Finnish/Men/Low fitness |
N/A |
9/4
|
| *Cardiff University Critical Appraisal Checklist: Specialist Unit for Review Evidence (SURE)14 |
| Supplemental Table 9. Summary of Findings (Observational Analyticals) |
|
Author/Year (Study)
|
Population/Age/Ethnicity Investigated |
Diagnoses? |
Cardiff University Critical Appraisal Checklist: SURE Score* |
| Lorentzen et al41 |
Adults in suburban districts of Oslo
|
|
12/14
|
|
Hellsten et al42
|
Underserved/ minority populations/Females |
|
|
| Paxton et al43 (Cross-sectional) |
Adult women/Hawaii (United States) |
N/A |
12/14
|
|
Dishman et al44 (Longitudinal; Cohort)
|
Adults/Hawaii (United States)
|
N/A
|
9/14
|
| Lippke et al45 |
“Adults” |
|
9/14
|
|
Stoltz et al46
|
Adults in weight loss groups and activities
|
|
9/14
|
|
Plow et al47 (Survey)
|
Adults
|
N/A Multiple sclerosis
|
11/14 |
| Fortier et al48 |
Adults |
Type 2 diabetes |
11/14
|
|
Dishman et al49
|
University Students/United States
|
N/A
|
9/14
|
|
Geller et al50
|
Adult/Hawaii (United States)
|
N/A
|
9/14
|
|
Bernard et al51
|
University students/France |
N/A
|
13/14
|
| *Cardiff University Critical Appraisal Checklist: Specialist Unit for Review Evidence (SURE)14 |
Processes of Change
The POC were measured by self-report questionnaire and assessed by two (2) of the five (5) studies included in this review.16,17Additionally, included in both studies was a longitudinal comparison of the POC from baseline to follow-up.16,17
Quantitative Measures
Objective quantitative data regarding physical activity was collected by three (3) of the five (5) studies in this review.16,19,20 However, two (2) of these included self-report daily exercise logs,16,19 and one (1) used functional fitness measures.20
Observational Investigations (Descriptive and Analytical)
Sixty-one (61) observational studies, classified as either descriptive or analytical following analyses with the SURE checklist, did not yield high-level evidence and therefore, conclusions could not be derived from their results. Despite this level of evidence, only the studies of low rigor (n=31) were omitted completely from the qualitative aspect of this review. The remaining thirty (30) observational studies were of low to moderate quality, including eleven (11) observational analytical designs and nineteen (19) observational descriptive designs.
Supplemental tables describing populations and diagnoses investigated. A descriptive assessment has been included to meet the aims regarding identification of populations and topics investigated in the past ten (10) years regarding the TTM (Supplemental Table 8 and Supplemental Table 9).
DISCUSSION
Similar to systematic reviews performed before 2008, this review has combined a quantitative and qualitative approach without meta-analysis due to variation in reported outcomes. Lack of measured and reported effect sizes results in an inability to quantitively combine results.7,8 Of the literature conducted in the last ten-years (2007- 2019), five (5) interventional type studies were found to be of adequate methodology and quality for this review. Assessing the results described above, the stages of change is the first construct to be analyzed.
Stages of Change
An accurate and consistent assessment of the stages of change construct is important for a true stage-matched intervention. Two (2) of the five (5) studies assessed SOC via means which were unvalidated.18,19 Two (2) of the remaining studies utilized SOC questionnaires and reported current research on reliability and validity.16,17 Additionally, one study utilized an exercise status questionnaire utilized in 1997.20
Overall, for the SOC construct, quasi-experimental studies and randomized controlled trials, alike have not contributed new data regarding stage changes than had been reported prior to 2007. This appears to be due to failure to appropriately stagematch the interventions based on the TTM. Despite the support to the TTM provided by findings listed above from these studies, conclusions cannot be considered valid because within three (3) of the five (5) studies, the interventions and/or methods of assessment were not appropriate, therefore lacked internal validity.
As has been stated, interventions were not applied as proposed by the TTM-SOC. Only one (1) interventional study demonstrated appropriate, stage-matched measures and yielded moderate quality results and recommendations.16 Two (2) of the studies claimed to be stage matched, however, their methods and procedures were unclear to delineate that cognitive processes were used in contemplation, and behavioral processes in action and maintenance.17,18 One (1) of these investigations inappropriately applied an action-phase intervention to all subjects irrespective of the stage to which they were categorized. Specifically, subjects in precontemplation, a traditionally cognitive-based phase of the model, were given an action-phase intervention.18 Furthermore, one (1) study lacked appropriate stage-matching altogether, with one third of the participants in the contemplation stage performing the exercise intervention,20 rather than receiving interventions to address the cognitive processes needed to move to action.19 Results from both studies should be taken cautiously, as integrity to the model is questionable. This lack of internal validity limits the overall validity of findings.
Decisional Balance
Decisional balance (DB) was addressed in one (1) randomized controlled trial (RCT) and one (1) quasi-experimental study of the five (5) interventional studies included in this review.16,17 The first, by Findorff et al, reported no significant difference between a group with TTM-based intervention and control group. This finding is inconsistent with the theoretical basis of decisional balance within the TTM.16
Regarding the cumulative recent evidence on decisional balance, little to no support has been shown to favor the construct as it has been proposed with the TTM. Decisional balance has been omitted in trials based on the TTM regarding health behavior change.
Processes of Change
One (1) RCT and one (1) quasi-experimental study measured the POC.16,17 According to results found in the RCT,16 exercise adopters demonstrated increased use of behavioral processes and decreased use of cognitive processes, consistent with the TTM and displaying positive support for the POC construct. In this same study by Findorff et al, individuals who progressed in the stages but were not yet in action (exercise readiness), demonstrated decreased cognitive scores.16 This additional finding supports the POC construct proposed in the TTM.
Overall, there has been mixed findings between the two intervention studies regarding the POC construct. Findorff et al. measured these processes to be in support of the TTM, whereas findings by Fischer and Bryant did not.16,17 In a continued trend, this construct also appears to be neglected by researchers when implementing TTM-based interventions for behavior change.
Self-Efficacy
One (1) RCT and one (1) quasi-experimental study in this review measured SE for exercise among their participants.15,16 The first of these studies found SE to be a significant predictor of whether a person would become an exercise adopter in the long-term.16 With a comparison between two time periods, the exercise readiness group demonstrated decreased SE at follow-up.16 Contrary to the TTM, this study also found SE scores for exercise adopters to decrease when measured post-intervention as compared to their prior scores.16
Self-efficacy is an additional construct which appears to be inconsistently measured with interventions relating to the transtheoretical model. Based on the literature cited above, recent research has mixed findings which both support and negate the construct within the TTM.
Objective Measures of Physical Activity
Three (3) of the five (5) included interventional studies included subjective assessments of physical activity (PA).16,17,18 One (1) additional study appeared to consider the ‘action’ stage of change as its primary measurement of achieving PA criterion.19 In one RCT, exercise behavior was exhibited among participants of the experimental group, who became exercise adopters significantly more frequently than the control group.16 In another RCT, an exercise group receiving exercise consultation interviews as a TTM-based intervention, demonstrated significant change in PA levels from baseline to follow-up at 6-weeks.18 A significant difference between PA levels was also present when comparing the experimental and control groups, congruent with the TTM.18
The summative data of recent years on objective PA measures with TTM-based interventions is directed towards subjective measurements of PA. Positive support for the model has also been demonstrated, with these subjective measurements, with the association between increased PA levels or exercise adoption and a TTM-based intervention.16,18
Overarching findings of this review allude to a continued omission of multiple constructs of the TTM with its implementation for exercise behavior change. As was found in the research published by Bulley et al7 and Hutchinson et al,8 the TTM continues to be inconsistently tested within interventional studies with failure to achieve a true stage-matched intervention. Furthermore, the SOC construct continues to be the singularly emphasized measure among interventions despite the previous recommendations for holistic/full implementation of the model.
A limitation of this review is due to the limited strength of methodology among the studies investigated. Moderate was the highest quality of evidence available. Significant limitations to some of the investigations reviewed included improper stage matching interventions, self-report with recall bias and unclear description of methodologies regarding stage matched interventions. Though it is difficult to use every construct of the model due to required increase of sample size as variables are added, the lack of assessment of the entire model, is a limitation of recent TTMSOC literature.
Objective measures of PA have not been cited as a construct of the TTM-SOC. However, based on the model’s recent application for health behavior change, specifically for exercise, there must be impetus to require a measure beyond self-report for PA. The intervention investigations relied solely on self-report instruments requiring recollection of exercise, thus introducing recall bias.16,17,18,19 While Findorff et al16 utilized daily exercise logs, one (1) study measured exercise via questionnaires based on recollection of past events, and one (1) study inferred patterns of PA based on answers in the Stages of Change Scale.17,18 One investigation by Prochaska et al,19 was unclear in assessment of frequency and duration of exercise per week, although the authors appeared to consider achievement of the action stage of change for PA (30-minutes of exercise, 5-days per week) to be the equivalent to meeting criterion for that behavior. In a scientific effort to minimize bias, recall bias, and other errors associated with thinking, objective measures such as activity trackers and pedometers are a necessity to increase validity of findings.
CONCLUSION
Evidence added to the TTM-SOC model in the past 10-years does not appear to provide additional guidance for the health practitioner regarding a stage-based approach for PA. It appears that promotion of cognitive process in earlier stages and behavior processes in latter stages, as outlined by the TTM, has neither been negated nor supported.
Holistic assessment of all constructs of the TTM, including SOC, POC, DB, and SE for PA, were limited among the moderate to high quality of evidence, peer-reviewed studies published in the last ten years. As such, there can be no definitive conclusions with regard to the effectiveness of stage-matched interventions to promote a change from sedentary lifestyle to adoption of PA. There is a need for more rigorous research to be performed to test the application of this model for this behavior change and use of physiological and quantitative, measures for PA within future investigations.
Research conducted to-date has assessed behavior change, or adoption of the behavior of PA. Theoretically, the TTM-SOC was designed to explain the cessation of behaviors (Prochaska et al21). The application of the TTM-SOC to adoption of PA, appears to bypass cessation and move to adoption. Mechanism must be understood in order to measure and then manage a diagnosis or a process. Therefore, the application of the TTM-SOC to behavior adoption requires more specific investigation, such that the mechanism of cessation is considered with then the adoption of PA. Only then, would guidance for practitioners be translated with merit from theory to practice.
Therefore, future research is needed with assessment of SOC to cease sedentary lifestyle in addition to the SOC for PA adoption. A true test of the model with stage-matched interventions and use of all constructs must be done for validation with PA.
In an attempt to manage PA lifestyle and PA itself, researchers must devise a method of measurement with high validity and reliability. This should be possible with the current technology available, however, if PA continues as self-assessment, or unassessed, the evidence for the support of the TTM-SOC will remain questionable and of low evidence.
CONFLICTS OF INTEREST
The authors declare that they have no conflicts of interest.


