INTRODUCTION
Black widow spider is a rare type of spider that lives in moderate climatic conditions and is found in the rural area. Latrodectus Tredecimguttatus, sometimes known as the Mediterranean black widow, the European widow spider, or the steppe spider, is a species belonging to the genus Latrodectus. It is commonly found throughout the Mediterranean region.1
Widow spiders are shy and nocturnal. They usually bite when their web is disturbed or upon inadvertent exposure to shoes or clothing.2
In Albania, poisoning due to the bite of this specific type of spider was first observed in the early 19th century. The first reported cases of patients experiencing acute poisoning due to the bite of this spider were restricted to a limited area in the country including the western lowlands specifically the Kavaja, Durrës and Myzeqe areas. The cases of poisonous spider bites were more often reported from the month of July to September. The period over which the cases of spider bites were reported, was related to the life cycle of the spider and the increased human agricultural activities during this period resulting in a greater contact with the external environment. The map indicating the distribution of affected patients extended across the northern and southern regions of the country during the upcoming years, but was predominant in the plain and hilly areas. The natural origin of this causative organism is attributed to the transportation of the spider from the neighboring countries together with various goods, especially with vehicle tires.3
The clinical manifestations observed after a spider bite are variable and include abdominal pain, vomiting-nausea, headache, anxiety, itching, palpitations, and high blood pressure; however, pericarditis and myocarditis occur very rarely.4 The grading system classifies the severity of envenomation into three categories. The characteristics of Grade 1 envenomations range from no symptoms to local pain at the envenomation site with normal vital signs. Grade 2 envenomations involve muscular pain at the affected site causing a gradual migration of the pain towards the trunk, diaphoresis at the bite site, and normal vital signs. Grade 3 envenomations include the grade 2 symptoms with abnormal vital signs; diaphoresis at the bite site; generalized myalgias to the back, chest, and abdomen; and nausea, vomiting, and headache.2 Our patient experienced myocarditis resulting in pulmonary edema, hemoptysis as well as muscle cramps, itching, anxiety, headache, palpitations, and high blood pressure.
CASE REPORT
A healthy 17-year-old girl while moving the billowy bundle of straw was bitten by a spider in the middle anterolateral region of the right thigh. The patient lived in the village, Darëzezë, Fier region, Albania. In her family history, there were evidence suggesting that two adult men were bitten by black widow spiders in the previous years and were hospitalized (Map 1).
Map 1: The Geographical Location of the Fier Region, Albania.
Ten minutes after the bite, the patient experienced severe pain in the lumbar and abdominal region and numbness in both the feet. She was taken to the emergency department of the regional hospital and was hospitalized immediately. After 24 hours, her condition deteriorated and her vital signs altered. The aggravation of her symptoms indicating generalized pain, acute respiratory distress, vomiting, hemoptysis, tremor and agitation led her to be transferred to the university hospital.
Clinical examination of the patient indicated pale skin, diaphoresis, oral cyanosis, orthopneic position, pulmonary auscultation characterized by crepitations in the base of the lungs, rhythmic cardiac tones, and normal abdominal palpation.
Vital signs were as follows: blood pressure recordings at 110/60 mmHg: Pulse rate as 110 beats/min, respiratory rate of 21 breaths/min, oxygen saturation at 75%, and a physical state of consciousness, alertness, cooperativeness and agitation.
Laboratory findings were: White Blood Cell count of 31.8×103/mm3 (Lymphocytes 3.4%, Monocytes 2.7%, Granulocytes 93.9%), Red Blood Cell count of 4.78×106/mm3, Hemoglobin 13.8g/dL, Platelet 275×103 /mm3, Hematocrit value of 45.0%, Glucose level of 103 mg/dl, Urea level of 27 mg/dL, Creatinine value of 0.6 mg/dL, (ALT) alanine aminotransferase activity of 22 U/L, (AST) aspartate aminotransferase activity of 75 U/L, Amylase activity of 127 U/L, Lactat dehydrogenase activity of 426 U/L, Creatine kinase activity of 286 U/L, CK-MB range of 110 mg/dL, Troponin level of 31, 3 ng/mL, International Normalized Ratio 1.339, Potassium level of 3.6 mmol/L, Sodium level of 132 mmol/L. PCO2 of 44.8 mmHg, PO2 of 24.5 mmHg, pH 7.334, O2Hb of 47.0%, BE of -2.7 mmol/L, BEecf of -2.6 mmol/L, BB of 45.4 mmol/L, Osm of 293 mOsm/kg, H+ concentration of 46.4 nmol/L and PAO2 of 88.8 mmHg (Table 1).
| Table 1: Hematological and Biochemical Recordings of the Patient from Day 1 to Day 8. |
| Hospital Day |
Normal Range |
Day 1 |
Day 2 |
Day 3 |
Day 4 |
Day 5 |
Day 8 |
| White Blood Cell (×103/mm3) |
4.0-10.0 |
|
31.8 |
27.7 |
17.2 |
12.8 |
7.3 |
| Red Cell (×103/mm3) |
4.20-6.10 |
4.15 |
4.78 |
4.75 |
4.18 |
4.25 |
5.29 |
| Hemoglobin (g/dL) |
13.8 |
11.6 |
13.8 |
13.9 |
12.3 |
12.9 |
14.1 |
| Hematocrit (%) |
35.0-50.0 |
|
45 |
44.8 |
39.6 |
38.1 |
42.3 |
| Platelet (×103/mm3) |
150-390 |
361 |
275 |
267 |
237 |
243 |
257 |
| Glucose level (mg/dL) |
74-106 |
110 |
103 |
164 |
121 |
110 |
114 |
| Urea (mg/dL) |
|
28 |
27 |
28 |
30 |
38 |
35 |
| Creatinine (mg/dL) |
0.6-1.4 |
0.8 |
0.6 |
0.7 |
0.6 |
0.7 |
0.7 |
| Aspartate aminotransferase (U/l) |
0-35 |
13 |
75 |
82 |
71 |
51 |
42 |
| Alanine aminotransferase (U/l) |
0-45 |
21 |
22 |
24 |
23 |
21 |
22 |
| Lactate dehydrogenase (U/l) |
125-250 |
|
426 |
|
|
|
|
| Creatine kinase (U/l) |
0-171 |
|
286 |
|
|
|
142 |
| Creatine kinase-MB fraction |
0-24 |
|
110 |
|
|
|
36 |
| Total Bilirubin (mg/dL) |
0.3-1.2 |
0.78 |
0.6 |
0.6 |
0.6 |
0.9 |
0.4 |
| Total Protein (mg/dL) |
6.2-8.3 |
|
6.7 |
6.4 |
6.1 |
6.6 |
|
| Sodium (mmol/L) |
136-146 |
|
132 |
137 |
|
|
|
| Potassium (mmol/L) |
3.5-5.1 |
|
3.6 |
3.9 |
|
|
|
| Chloride (mmol/L) |
98-106 |
|
95 |
97 |
|
|
|
| Troponin I (ng/mL) |
0,000-1,00 |
|
31.3 |
23 |
|
3.9 |
0.841 |
| INR |
0.720-1.200 |
|
1.339 |
|
1.339 |
1.386 |
1.154 |
| AST: Aspartate aminotransferase; ALT: Alanine aminotransferase; INR: International Normalized Ratio. |
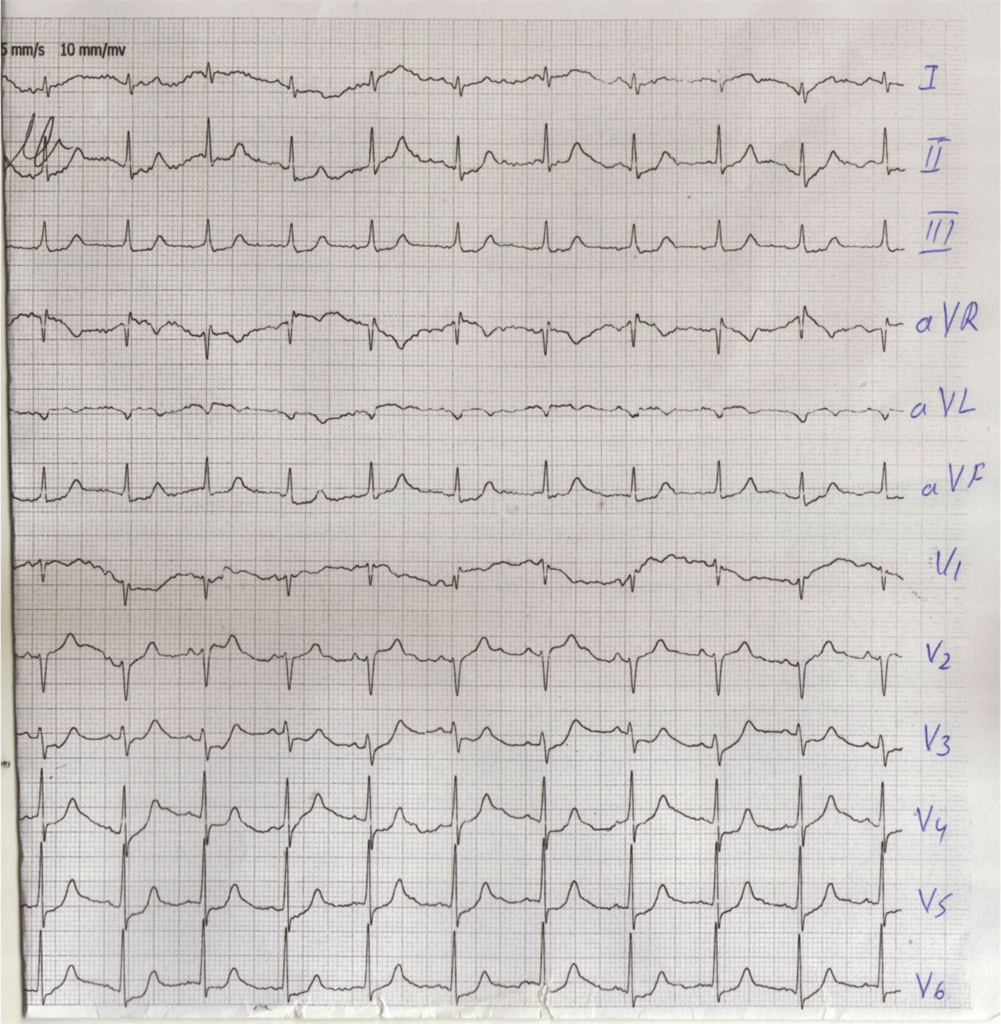
Electrocardiography results implicated modifications that mimic anteroseptal infarction and transitory changes of the repolarization phase. The electrocardiographic recordings of the patient showed a normal sinus rhythm, normal QRS axis, cardiac frequency of about 90 beats/minute, qS V1,V2,V3, subdenivelation of ST segment 2-3 mm V2,V3,V4,V5,V6 (Figure 1).
Figure 1: ECG 24 Hours after Spider Bite
Echocardiography results showed a normal left ventricle, modification in the segmental kinetics, hypokinesia of the medial and basal segments of the anterior wall.
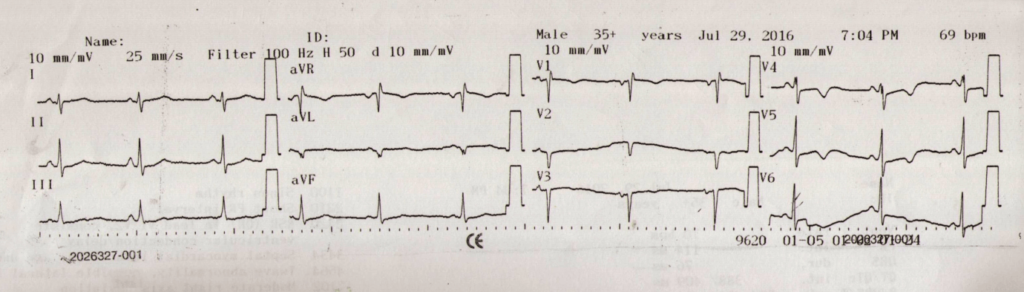
The medical condition of the patient improved following the administration of diuretics, anti-inflammatory corticosteroids, analgesic opioid drugs, electrolytes, intravenous perfusions, vitamins, antibiotics, hypnotic sedatives drugs and gastric protections. The normal troponin level was established six days following the spider bite (Figures 2 and 3).
Figure 2: ECG 48 Hours after Spider Bite.
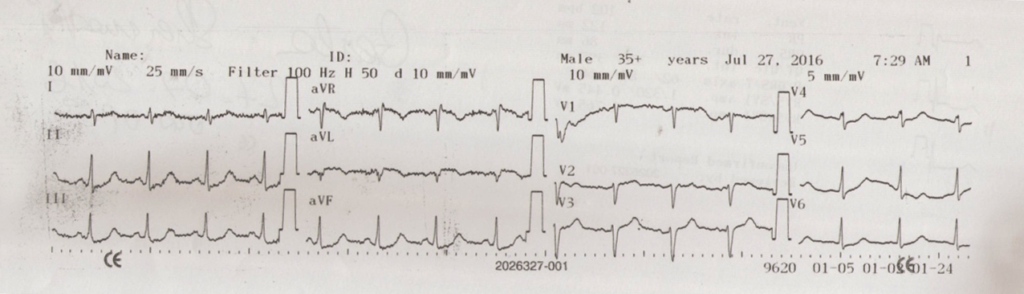
Figure 3: ECG 4 Days after Spider Bite
The patient was dismissed from the hospital after 10 days. The patient underwent routine checkup and echography conducted by the cardiologist.
DISCUSSION
Firstly, we discuss the kind of insect that bit the patient and its medical implications in the patient. Addressing this particular aspect of the study, we possess a clear anamnesis suggesting that the poisoning results from the black widow spider bite. In this particular case, the patient’s condition has been treated in the clinical context but the question arises as to whether the use of anti-venom could reduce pain and suffering, shorten the duration of envenomation, and reduce or eliminate the need for hospitalization.5
We strongly suspect that myocarditis was caused by the toxins and with the treatment of the clinical symptoms, the condition was reversed. The electrocardiogram (ECG) recordings signify the need of a differential diagnosis for the ischemic conditions of the heart, such as myocardial infarction or pericarditis. But the medical history of the patient, her young age, the increase in troponin levels and the echocardial findings relevant to her condition indicated impaired functions of the left ventricle function thus, resulting in myocarditis.
The differential diagnosis of myocarditis was suggestive of acute coronary syndrome, congestive heart failure, pulmonary edema and pulmonary embolism. Severe myocarditis in the present study was further complicated by pulmonary edema on account of low cardiac output. Prognosis for acute myocarditis can be accurate depending on the clinical presentation of the left ventricle ejection fraction and the pulmonary artery pressure. Our case study describes the whole chain of events occurring in the affected patient with a favorable diagnosis and cure.
CONCLUSION
Acute myocarditis can occur very rarely after a spider bite. The ECG changes are a modification of the Quality Real Service (QRS) complex mimicking acute myocardial infarction and transitory changes of the repolarization phase. The elevation of myocardial injury markers [CkMb, troponin] as well as echocardiographic findings of segmental hypokinesia and low ejection fraction is compatible with acute/fulminant myocarditis. The aim of the pharmacological treatment of fulminant myocarditis complicated by acute pulmonary edema was to reduce the intensity of symptoms of cardiac insufficiency and neutralize the effects of the toxins released.
CONFLICTS OF INTEREST
The authors declare that they have no conflicts of interest.


