What is known about the topic?
Global perceptive ambulance utilization is increasing annually, with previous research suggesting numerou underlying factors.
What does this study add?
This study will be emphasized on the role of public health with the support of primary research (Cross-sectional study) and secondary research (literature review). These factors have not been previously synthesized in the international literature. This narrative review clearly articulates the underlying problems.
What are the implications for practitioners (Both ambulance services and public health)?
This study outlines the need for further research of the causes of increased emergency ambulance utilization, to enable the development of appropriate strategies to manage misuse of ambulance services in the future.
INTRODUCTION
Overview
The primary role of all ambulance services is emergency pre-hospital medical care, although they generally provide both emergency response and patient transfer on behalf of the health sector. They provide easy access to health services, particularly out of hours, and contribute significantly to telephone triage and telephone health services through sophisticated communications infrastructure. In recent times it has become apparent that increasing health system pressures cannot be resolved only by adding resources but must also be addressed with new methods of service delivery.
The ambulance service is ideally placed to be part of the first line in the continuum of healthcare, and can significantly contribute to ‘treat and transfer’ or ‘treat and leave’ programs. If ambulance services can develop towards an out-of-hospital, clinical care service rather than merely pre-hospital clinical care, they could substantially add to the functionality of the health system. This could be through more efficient transfer of patient information; more efficient movement of patients; an ambulance service with public service – rather than profit-driven – philosophy; and patient treatment regimens consistent with the broader health system.
By integrating ambulance services into the health system generally, their respective strategic agenda is aligned, increasing efficiency, and providing an opportunity for an ambulance service, with its relevant expertise, to influence the outcome of ‘health’ initiatives.
The Problem Statement
Demand is growing throughout healthcare services, but for ambulance services, the increase is faster, in some countries close to twice the rate of other healthcare services and often without a commensurate increase in resources. Life expectancies are increasing, as is the frequency of serious adverse health events, multi-morbidity, and chronic diseases.1
Aging is not the only causal factor for increased emergency medical service (EMS).1 It has also been argued that, among all the conveniences of modern society delivering instant gratification to the door at the push of a button, there may be an increased expectation for an in-house health service in public perception. Such expectations, combined with the belief in quicker care when arriving at a hospital via ambulance services, could contribute to the growing volume of non-emergency ambulance calls, placing an increasing strain on ambulance services.
This kind of societal change and increased patient volume, combined with exacting government targets, requires ambulance services to achieve more, for more people (and, frequently, with the same or even fewer resources, as in the case of e.g. the National Health Services (NHS) in the United Kingdom (UK). In addition, the increased load exacerbates problems further down the treatment pathway, such as hospital overcrowding and Emergency Department waiting times. This in turn can cause increased ambulance handover times and further decrease the available ambulance cover, leading to states of severe under-resourcing, excessive workload, and dangerously high response times.
Given this state of increasingly stretched resources, limiting systematic over-triage leading to immediate ambulance response in low-acuity cases (were dispatching an ambulance car provides little or no patient benefit compared to viable alternatives) is vitally important, as over- triage potentially leads to shortages in high-acuity emergencies, increased response times, and other aspects of suboptimal EMS resource utilization. However, avoiding under-triage, i.e. inappropriately low response in high-acuity emergency cases, is even more important if medical ethics is to be respected.
Description of the Emergency Care Pathway
For our case study, the emergency care pathway consists of the Ambulance Service bringing a patient to the hospital (typically two paramedics in an ambulance), the emergency department (ED), and hospital departments that receive patients from the ED. Figure 1 shows the resulting process emergency care pathway suggested by World Health Organization (WHO).2
Figure 1. Emergency Care Pathway by WHO2
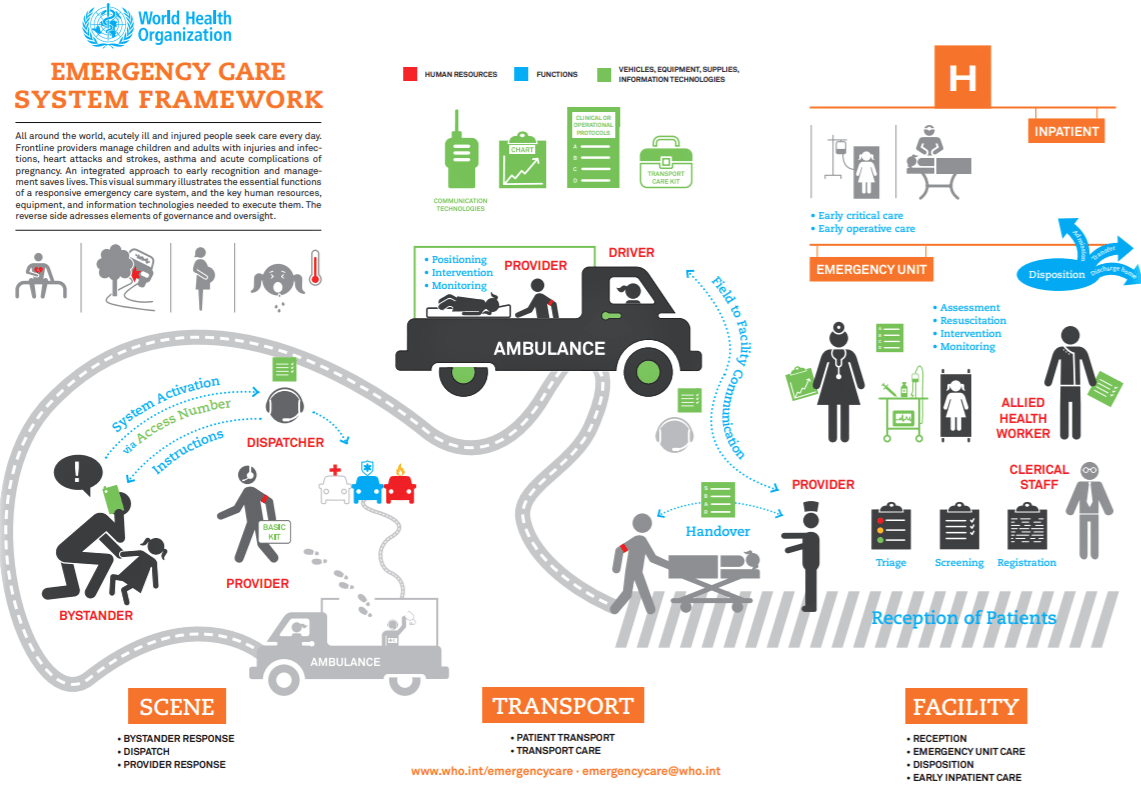
It is internationally recognized that there are 10 steps required for an emergency medical service to receive a call, respond, treat, transport the patient, and be ready and available for the next call. This requires all aspects of the service to work together in performing their roles in a manner that will ensure the total management of the call is done effectively and efficiently. The success of a call for assistance is the united effort of all staff.
This policy and procedure will detail all the roles and responsibilities required to complete all Steps in EMS call management. Specific ambulance policy, policy statements and procedures may be issued in support of specific actions within this management process.
What is the Public Health Connection to Ambulance Services?
Public health is an amazingly broad discipline that includes injury prevention, disease surveillance, meeting the needs of underserved populations, and much more. The American Public Health Association (APHA) has no less than 31 interest areas and or sections for its members, spanning from human immunodeficiency virus infection and acquired immune deficiency syndromes (HIV/AIDs) to school-based health to health information systems to behavioral health. There is even an emergency health services section concerned with ambulance services and emergency care systems. Table 1 has eventually prepared to demonstrate the common purpose where public health and ambulance services can work together for the development of the healthcare system not just in emergency care but also in preventive measures for preparation, prediction, and promotion.
| Table 1. Common Purpose of Public Health and Ambulance Services |
|
Purpose of Public Health
|
Purpose of Ambulance Services
|
| Prevention |
Prevent epidemics and spread of disease |
Play vital role in communicable and non-communicable diseases especially in secondary and tertiary prevention of Public Health |
| Protect |
Protect against environmental hazards |
Support the purpose of Public Health |
| Prevent |
Prevent injuries |
Injury surveillance system |
| Promote |
Promote and encourage healthy behaviors |
Promote community care services, when to call the ambulance and what to do in case of a medical emergency |
| Response |
Respond to disasters and assist communities in recovery |
Play a major role in all phases of Disaster |
| Assure |
Assure the quality and accessibility of services |
Assure the quality and accessibility of emergency medical services |
As a general rule, public health is a catch-all discipline that is concerned with the health of communities in general. As a result, it is essentially anything health-related that is not an individual healthcare service. Despite its broad mission, public health (Figure 2) is only a fraction of the healthcare system, especially in the United States (U. S.) where we have a substantial focus on acute care services.
Figure 2. The Public Health System Integrated with Ambulance Services
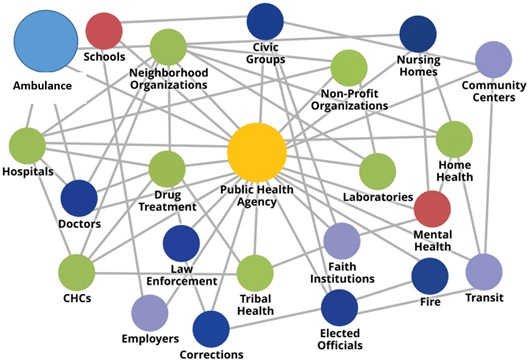
The history of public health is extensive and includes many great successes regarding environmental health, the control of infectious diseases, occupational health, and reductions in smoking amongst the general public. Public health is often a governmental responsibility and is accomplished to varying degrees at all levels of local, state, and federal government. At the federal level, multiple agencies, including the U.S. Public Health Service and the Centers for Disease Control and Prevention (CDC), have public health responsibilities. Every state has a health department, as do almost all counties and many larger municipalities.3
Research Questions
The research questions for this study were:
1. Does the public perception affect the inappropriate use of ambulance services?
2. Assess the knowledge among the community awareness of when to call an ambulance, know the role of ambulance services in society?
3. Does the community aware of the misuse or inappropriate use of ambulance services and how does affect the ambulance services?
4. Can public health play a vital role to reduce the inappropriate use of ambulance services?
Objective
The purpose of this study is to evaluate the public perception of appropriate usage of ambulance services and determine the applicable role of public health to reduce the inappropriate use of an ambulance.
METHODOLOGY
Study Design
A cross-sectional study was conducted to collect data from the general public using an online survey. The survey contains 9 questions that evaluate the public awareness of appropriate ambulance use. Participants are residents from United Arab Emirates (UAE) public within the age of 18 and above.
Sample Size
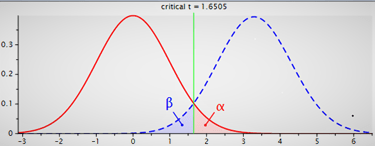
Used the t-tests for sample size selection. The minimum sample size required is 54 as below stated. However, a total of N=97 of participants’ responses were used to analyze the data as Figure 3.
Figure 3. Two Tails by Using t-test
| Sunday, April 14, 2019- 14:28:193 |
| t-tests |
Purpose of Public Health
Purpose of Ambulance Services |
| Analysis |
A priori: Compute required sample size |
| Input |
Tail(s)=Two
Effect size d=0.5
α err prob=0.05
Power (1-β err prob)=0.95 |
| Output |
Noncentrality parameter δ=3.6742346
Critical t=2.0057460
Df=53
Total sample size=54
Actual power=0.9502120 |
Inclusion Criteria
Complete surveys and answer data using the English language.
Exclusion Criteria
Uncompleted surveys, and answered with other languages.
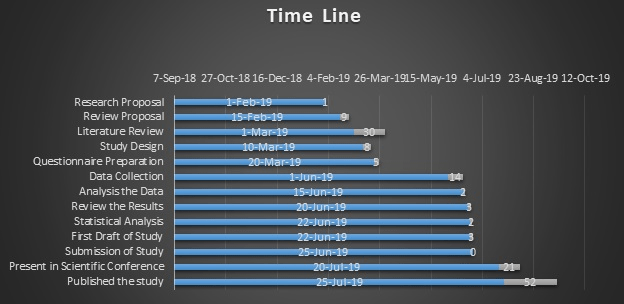
Study Period
The study has conducted within 5-months of duration (1 February 2018 till 30 June 2019).
Data Collection Tools
Data was collected through an online survey from the residents of the UAE.
Ethical Consideration
All the data collected online as well all the participants informed that anonymity and confidentiality of responses are guaranteed. The purpose of the study has been mentioned to participants as well the Institutional Review Board (IRB) approval is not needed.
Pilot Study
A pilot study has been conducted on a small scale to evaluate feasibility, time, cost, and improve upon the study design before a performance of a full-scale research project.
Data Entry
All data entered online by the general public voluntarily, a total of 97 responses received with 100% completion of the survey, and the average time has taken 2 minutes 27 seconds to complete the survey.
Data Analysis
Statistical Package for the Social Sciences (SPSS) and Microsoft Excel are used for statistical data analysis.
Methodology-Secondary Research
Literature review: The following Databases that were searched were MEDLINE, Literature (CINAHL), Cochrane library, Google Scholar, and PubMed. The search strategy was perused with key terms such as “ambulance Services and public health”, “misuse of ambulance services”, “public health role in ambulance services”, “demand of emergency medical services” and “scope of public health in EMS”. Additional articles were found from the reference list of these studies.
E.g. of PubMed Search Results (“ambulances” [MeSH Terms] OR “ambulances” [All Fields] OR “ambulance” [All Fields]) AND services [All Fields] AND (“public health” [MeSH Terms] OR (“public” [All Fields] AND “health” [All Fields]) OR “public health” [All Fields]).
Inclusion criteria consisted of full-text articles, studies conducted on ambulance services and public health relations, articles published in the english language from the period of 2002-2019. Peer-reviewed articles were preferred.
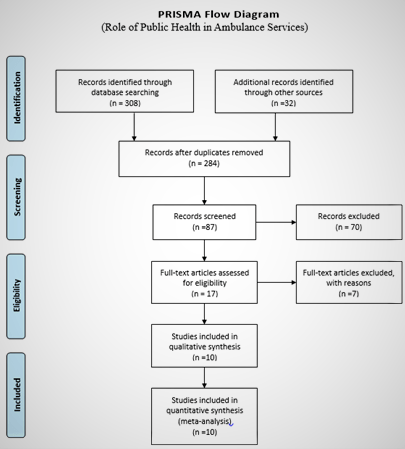
The search was broadened to in healthcare settings due to the lack of evidence found on ambulance services and public health. The articles were then reviewed by title and abstract. Irrelevant articles were excluded. The method sections of the articles were reviewed and study design literature reviews were preferred.The initial search resulted in 308 hits (Figure 4). Two hundred and twenty-one (221) were excluded due to unobtainable full-text articles and some were irrelevant based on title and abstract. Some were repeated articles. Eighty-seven (87) were then selected for further review. Upon inspection and thorough reading of the papers, 70 more were excluded. Finally, only 10 articles remained which matched the search strategy and inclusion criteria.
Figure 4. Prisma Flow Diagram used for Articles Selection to Conduct a Literature Review
RESULTS
Results for Primary Research
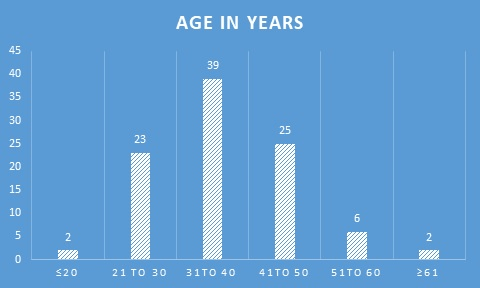
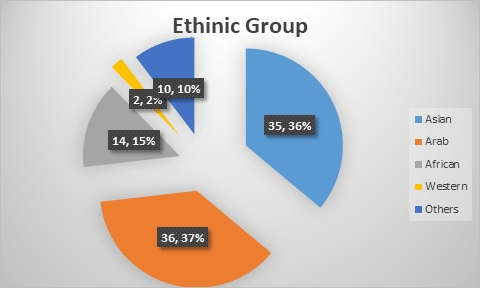
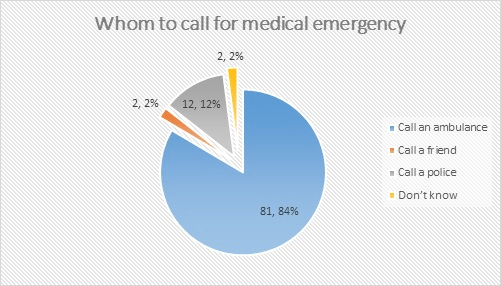
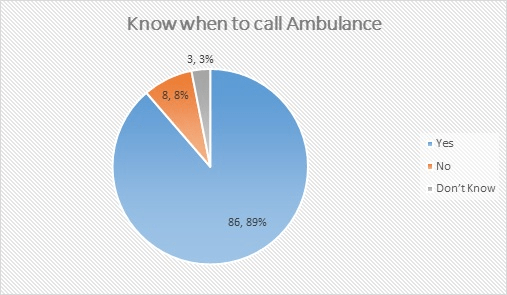
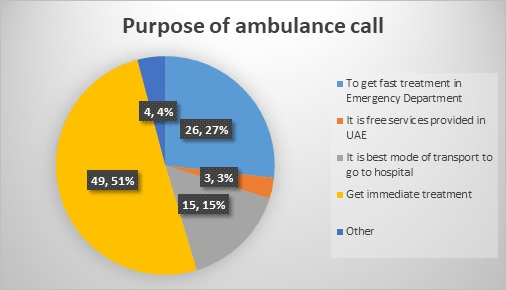
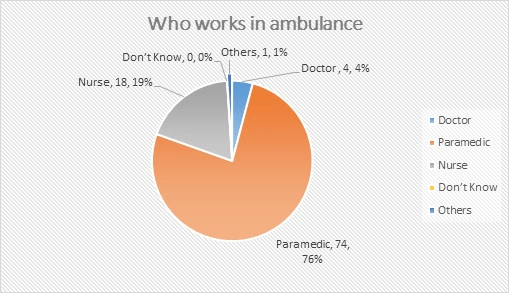
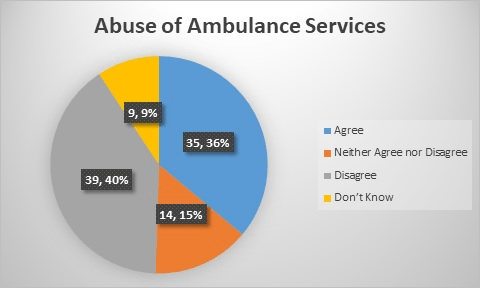
During the online survey, a total of n=97 (100%) participants enrolled voluntarily. The mean age of the participant reported was 41.5-years and further age distribution is mentioned in Graph 1. Among this survey almost n=39 nationalities participated those are residents of the UAE, thus they further cluster as a group in Graph 2 based on race. The majority of the residents are aware of when to and whom to call in case of a medical emergency in UAE (Graphs 3 and 4). The purpose of calling an ambulance is classified in Graph 5. The understanding about ambulance professionals is distributed in Graph 6 as per community perception. N=35 (36%) of the participants believe that ambulance services are misused referred to Graph 7 (Table 2).
Graph 1. Age Group
Graph 2. Distribution of Participants According to Ethnic Group
Graph 3. Perception of the Community Whom to Call in Case of a Medical Emergency
Graph 4. Perception of Community When to Call an Ambulance
Graph 5. Perception of the Community Why Need to Call an Ambulance
Graph 6. Perception of the Community Who Works in an Ambulance
Graph 7. Acceptance of Abuse of Ambulance Among the Community
| Table 2. Results for Secondary Research |
|
Authors
|
Year of Publication |
Study Design |
Study
Participants |
Study Settings
|
Major Findings
|
| Sultan et al4 |
2018 |
Cross-sectional retrospective |
N=801 |
Out of hospital |
A common reason for the utilization of ambulance services |
| Phung et al5 |
2018 |
Semi-structured interview |
N=16 |
Out of hospital |
Community first responders role in supporting ambulance services |
| Phung et al6 |
2017 |
Systematic scope review |
More than n=2000 articles |
Out of hospital setting |
Community responders scheme in the United Kingdom in collaboration with ambulance services. |
| Victor et al7 |
1999 |
census |
N=623000 |
Out of hospital setting |
60% of patients needed to call an ambulance while
remaining of the 40% should use other healthcare services rather than using ambulance services. |
| Gray et al8 |
2007 |
retrospective review |
N=354 |
Out of hospital setting |
|
| Stirling et al9 |
2007 |
Qualitative data were collected from semi-structured interviews |
NA |
Out of hospital setting |
Increased interactions between ambulance services and rural communities with an overall benefit to health care |
| Toledo et al10 |
2013 |
A cross-sectional survey |
N=911 |
Emergency
Department |
Community call ambulance for getting higher priority at the ED (34%), not having a car (34%), and financial concerns (17%). |
| Roberts et al11 |
2014 |
two mixed-methods studies |
NA |
Out of hospital setting |
Findings that explore the liminal and complex role of the first responder as both ‘practitioner’ and community member. |
| Palazzo et al12 |
1998 |
retrospective review |
N=300 |
Accident and
emergency department |
15.7% were inappropriate ambulance calls. |
| Møller et al13 |
2015 |
Descriptive analysis |
N=211,193 |
Emergency medical dispatch center |
“Unclear problem” was the most frequent category (19 %). |
DISCUSSION
Most of the ambulance services concerned a large increase in calls, and especially treating on the scene or treat and refer another healthcare facility rather than transferred by ambulance. Most of the ambulance services have given response time as key performance indicators, hence the emphasis on response times and transportations to an end destination, there may be a major underestimation of the value and cost-effectiveness of activities at the scene. This emphasis was reinforced by the performance measurement regime being concentrated on response times. However, the majority of the developed countries do not just emphasize response time only as key indicators they are promoting the clinical outcome indicators, as well-focusing on prevention of medical emergency and involvement of community volunteers. Moreover, we would argue that the process of developing new indicators should be deliberative and involve wide a range of stakeholder’s e.g. healthcare organizations, law enforcement. The major concern here is the knowledge gap between healthcare professionals and their patients which means that the concept of the perfectly informed customer central to classical economics is absent. It may well-be that the problem of information identified is the key obstacle to the closer involvement of the public in this process.
Our findings about public perceptions of ambulance services when to call for an ambulance in case of emergency is the biggest challenge. Patients describe their experience of the situation as “intolerable” and cite feelings of anxiety before calling.14 Booker et al14 study of patients who called an ambulance for primary care problems revealed a misunderstanding of options in the healthcare system or previous negative experiences seeking care as factors influencing the decision to call, which is consistent with the cues we found that paramedics use to identify a patient’s inability to cope.
This study also builds on previous studies that have examined the perceived prevalence of inappropriate use by community. These empirical studies of inappropriate ambulance use have focused primarily and often solely on clinical criteria. Our examination of how paramedics view and judge appropriate versus inappropriate ambulance use found that paramedics also tend to characterize the appropriateness of ambulance use according to contextual information gathered on scene.
Ultimately, addressing the problem of ambulance misuse requires asking fundamental questions about what the role of paramedics and ambulances should be in the healthcare system. In the UAE the context, the patient initiates ambulance use, and paramedics are unable to refuse transportation or to transport patients to alternative care settings. In addition to the patient attributes noted in this study, more research is needed about the effect of organizational and systemic factors on ambulance use and perceptions of appropriateness.
The biggest challenge is to “educate the public” in terms of recognizing a real medical emergency and to males aware of “when to call an ambulance”. The ‘public’ served by the emergency services is varied as is the range of activities; the public’s perceptions of the role of the service may be inherently simple and conservative; and the culture of the service itself may also be conservative and at times defensive in its approach to the users and conflictual in its relationship with other healthcare professionals with their aims, objectives and performance measures to fulfill.
This present situation of increased workload of ambulance services and misuse of ambulance services can be tackled with “public health initiatives”. Thus public health policies, the modern health system, and community awareness are vital to consider for a successful integrated healthcare system.
LIMITATIONS
The major limitation of our study is the small sample size (99 participants only) so the results cannot be generalized.
STRENGTHS
• Overall study has shown positive results that majority of the participants are aware of when to call and whom to call in case of medical emergency.
• The study had provided more detailed information to explain complex issues related to misuse of the ambulance services.
• Data collection is usually cost efficient for this study.
• The study as well as suggests exploring the individual items to understand public perception for utilization of ambulance in more depth.
CONCLUSION
In case of medical emergency the ambulance services is the first choice for the global community, however calling an ambulance still a huge dilemma. This study emphasizes almost 35% of participants believed abuse of ambulance services, though there might be numerous reasons for calling ambulances unnecessary. We can change this perception of the public by completing the healthcare system approach and adopting the public health strategies. The basic steps can be adopted by “public health education initiatives” in collaboration with ambulance services and public health together to reduce the workload of ambulance services, train the community for recognizing the medical emergency, promote the culture of health prevention and share the knowledge when to call an ambulance.
We as a global community need to acknowledge that there is a need for further research in the development of policies, procedures, and collaboration for the enhancement of ambulance services.
RECOMMENDATIONS
Given that, many strategies could help reduce the number of inappropriate calls including:
• Public Awareness: Raising awareness of the public about “when to call an ambulance initiative” can make a huge difference and public health can play a vital role through the journey of the patient in case of a medical emergency.
• Collaboration between Public Health Organization and Ambulance Services: From prevention, protection, promotion till post-treatment and rehabilitation both public health and ambulance services can work together.
• Education Institutes: Education institutes need to consider teaching curriculum in medical schools, paramedic schools, or other allied healthcare colleges to consider the importance of the role of public health and ambulance services in our community.
• Global healthcare organization: WHO and Ministry of Health of respective countries can develop the “Global Public Health Strategy” to reduce the inappropriate calls of ambulance services.
ACKNOWLEDGEMENTS
I wish to thank all the participants who gave their time to participate in the study and the reviewers for their time and constructive feedback.