INTRODUCTION
A distal clavicle fracture is a relatively uncommon injury.1 When a distal clavicle fracture occurs, there is usually elevation of the medial part of the clavicle as the lateral fragment is held in place with the acromioclavicular (AC) capsule. Hereby, we present a case of a 22-year-old male with an unusual fracture dislocation of the distal clavicle.
Patient
A 22-year-old male presented himself at the emergency room with pain at the right shoulder after a motor-bike accident. He had fallen on his right shoulder when driving approximately 35 km/h. On physical examination, we found elevation of the distal clavicle with displacement of the medial part caudally. There was pain on palpation. The piano key test was negative. The skin was intact and without tension. Abduction and flexion of the arm were painful. Neurovascular examination of the arm was normal.
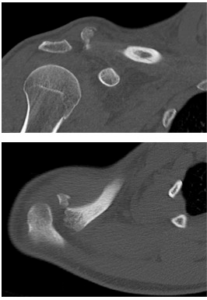
The radiographs showed a distal clavicle fracture with an apparent disruption of the AC joint (Figure 1). A CT-scan (Computed Tomography) was obtained because physical examination and the radiographs did not comply. The CT-scan showed an intact AC-joint with a Neer type II B fracture pattern, except for a dislocation of the medial fragment to dorso-caudal (Figure 2).2
Figure 1: Anteroposterior (AP) radiograph of the right clavicle.
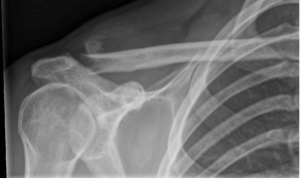
Figure 2: (A) CT-scan of the right clavicle showing an intact AC joint and (B) dorsocaudal displacement of the medial part of the clavicle.
Intervention
Ten days after the initial trauma, the patient was treated with open reduction and internal fixation using a hook plate (Figure 3). A dorsocaudal displacement of the medial part of the clavicle was seen. The fracture was reduced using reduction clamps and the hook plate was placed. Due to the small distal part, only screws medial to the fracture was placed. After the surgery the patient was allowed 90 degrees abduction and forward flexion of the right arm for six weeks.
Figure 3: AP radiograph of the right clavicle six weeks after open reduction and internal fixation using a hook plate.

Outcome
Six weeks post-operative the patient had no pain and full range of motion of the arm. He reported some loss of muscle strength with abduction. The hook plate will be removed in three months.
RELEVANT LITERATURE/DISCUSSION
A fracture of the distal clavicle is relatively uncommon. It accounts for approximately 10-15% of all fractures of the clavicle.1 There are two ways to classify a distal clavicle fracture: The Craig’s classification or the Neer classification.2,3 In both of these a type II distal clavicle fracture is unstable, where type II A occurs medial to the coronoid and trapezoid ligament and type II B occurs medial or lateral to the trapezoid ligament where either the coronoid ligament is torn exclusively or both ligaments are torn. In both classifications the medial part of the clavicle is elevated. None of the classification describes dorsocaudal displacement of the clavicle. In this case there was probably a blow to the shoulder, which pushed the medial part of the clavicle caudally where it became captured under the distal fragment. The X-ray in this case was misleading, appearing as a disruption of the AC joint. To our knowledge, this has never been published before. We obtained a CT-scan because the Xray did not comply with physical examination. The risk of a misleading X-ray is either malunion of the clavicle in conservative treatment, which can lead to shoulder complaints or unexpected finding during surgery, which can complicate the operation.4
Due to the risk of non-union and the young age of the patient an operation was planned. Although this type of fracture (and the operative possibilities) is already described by Neer in 1963, till this date there is no universally agreed standard operative procedure for displaced distal clavicle fractures.5 We found two reviews and a meta-analyses concerning the treatment of a distal clavicle fracture. Oh et al, found no statistical differences in union/non-union rates but more complications in the group treated with a hook plate or Kirschner wires in combination with Tension Band Wiring (TBW).6 They advised using intramedullary screw fixation, CC stabilization or interfragmentary fixation. Although they do state that the results should be interpreted with caution, ‘as the validity of the observational studies is limited by the lack of a control group (case series), imbalances between the comparison groups because of the lack of randomization (retrospective case control studies), and potentially biased assessment of out- come measures due to the lack of blinding’. Sambandam et al5 stated that all techniques give good functional outcomes, but flexible and semi-rigid fixation like open or arthroscopic coracoclavicular (CC) fixation, tension banding with sutures and coracoclavicular screws seem to avoid most of the implant related secondary complications.5
Also in this review, they state that the level of evidence is low. Stegeman et al7 stated that a hook plate is the most frequently used fixation technique, although it has the highest complication rate compared to intramedullary fixations and sutures.
RECOMMENDATIONS
In case of inconclusive physical examination or radiographs of a distal clavicle fracture, we advise to obtain a CT-scan. There is no optimal treatment for distal clavicle fractures. We advise a critical assessment of individual case. Until more research is undertaken, the best treatment is the surgical technique in which the operating surgeon is most experienced and familiar with.
CONFLICTS OF INTEREST
The authors declare that they have no conflicts of interest.
CONSENT
Since we did not add photographs in which the patient was recognizable, we did not obtain informed consent.


