BACKGROUND
Every summer, Berkshire plays host to a large event that attracts over 100,000 attendees for a weekend of merrymaking.1 Hosting such a large group of attendees comes with several considerations, one of which is access to medical attention. The local hospital in Berkshire is a district general hospital which has approximately 1000 beds and serves a population of around 500,000 people. It has a well-established emergency department (ED). Attendances to EDs have been increasing annually. This is accompanied by increased pressures, waiting times and need for resources.2 When the population abruptly increases by 20%, measures need to be put in place to manage the demand on healthcare services to ensure that all patients receive safe and effective care both in hospital and pre-hospitally.
METHODS
An annual review of event-related attendances to the ED has been carried out since 2013 to identify key trends in patient presentations so as to educate, plan and guide the pre-hospital and hospital response for the following year.3 Staff recognised that the ED was busier during the weekend of the event as there was the footfall of patients that self-presented to the ED as well as those that were referred by the event medical team. Key aspects that were analysed included: gender, age, mode of arrival, event medical assessment, type of presentation, length of ED stay and involvement of drugs or alcohol. Since the pandemic, another aspect that was assessed was whether the patient tested positive for coronavirus disease-2019 (COVID-19). Any patient who came to ED from the event were included in the data. As the demands on ED continue to increase each year, it became apparent that planning within the ED, pre-hospital team and communication with event planners were vital to enable all patients to receive high quality care. This data provided the hospital and pre-hospital team with objective analysis of changes made to see if they reduced the demands on ED.
RESULTS
Figure 1 shows the number of event-related attendances to the local ED since 2013, when data analysis was started. In 2013, just under 100 patients presented to ED, compared to just under 75 in 2022. Overall, event-related attendances decreased over the years.
Figure 1. The Number of Event Related Attendances to ED
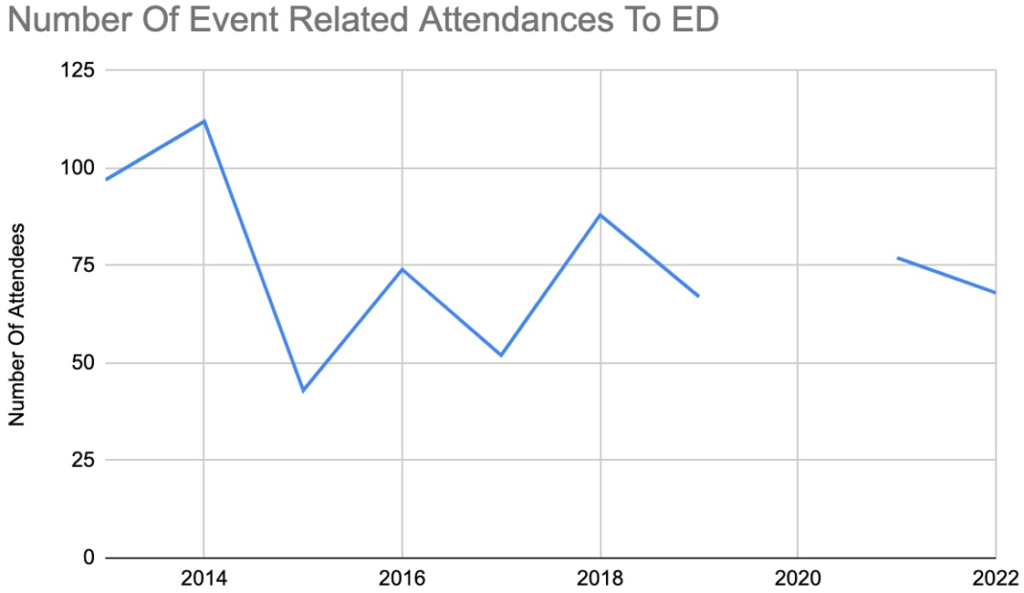
N.B. The event did not take place in 2020 due to the COVID-19 pandemic.
In 2013, approximately 50% of attendees requiring medical attention used the medical facilities at the event prior to booking into the local ED (Figure 2).4 This steadily grew through the years to approximately 65% in 2022 as more attendees recognised the availability of the pre-hospital care they could receive. Thereby, reducing the demand on the local ED as most patients were able to be seen and discharged pre-hospitally.
Figure 2. The Percentage of Patients Seen by the Event Medical Team Prior to ED Attendance
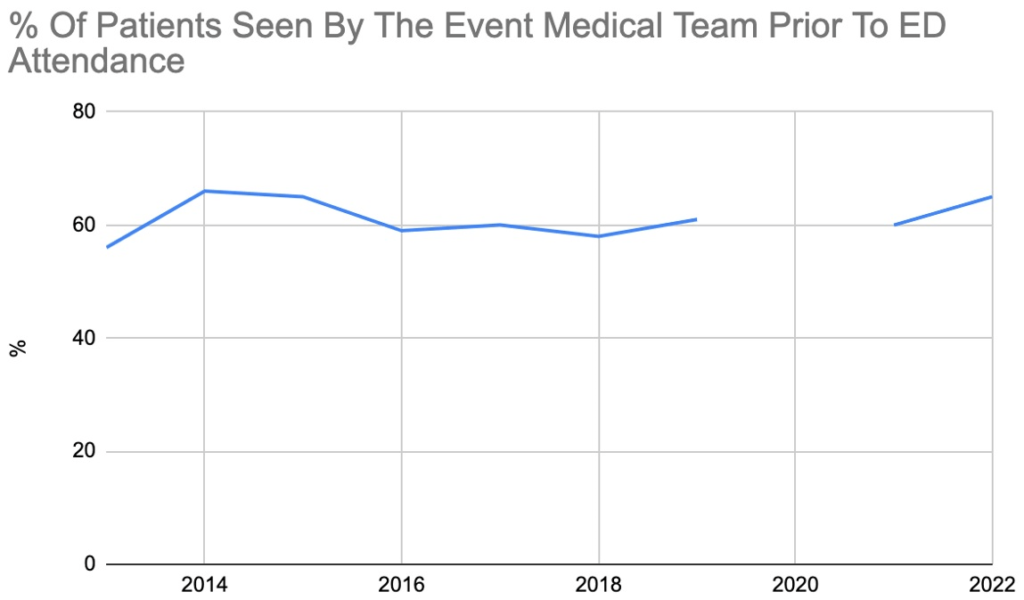
N.B. The event did not take place in 2020 due to the COVID-19 pandemic
Over the years of study, the peak ED attendance time from the event was between 1800-2000. Fifty-seven percent (57%) of patients attended between the hours of 2200-0800. This coincided with the night shift when staffing levels were at its lowest. To alleviate this, the minor injuries unit remained open for extended hours and ED staffing levels (including doctors, advanced care practitioners, emergency nurse practitioners and nurses) were increased during the evening and night shifts. Therefore, improving patient care and safety.
Figure 3 shows the different types of presentations coming to ED. Annual analysis revealed that injuries, such as wounds, fractures or dislocations, were the most common presentation to ED. The second most common presentation was the combination of both alcohol and drugs. Several of these patients did have several reasons for presenting. For example, drug toxidromes causing supraventricular tachycardias. In 2014, 112 event attendees came to ED.5 A large number of patients coming to ED with injuries required manipulation under sedation, plasters or casts and referral to fracture clinic for follow-up. Time, multiple clinicians and resources were needed to manage these patients. To attenuate this, the event medical team were able to introduce X-ray capabilities and management of minor injuries pre-hospitally for subsequent years. This proved effective as in 2015, only 43 event attendees came to ED, a 62% reduction in patients from 2014. The introduction of these services led to a marked reduction in the number of injuries sent to ED, allowing staff to focus on other unwell patients.
Figure 3. Graph Representing the Number of the Different Presentations Since 2013
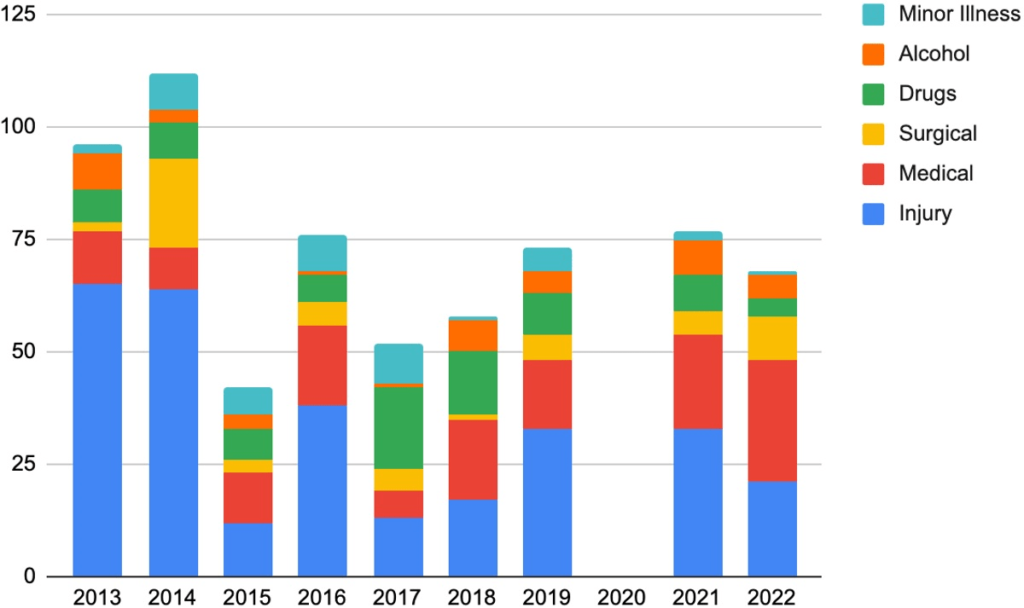
N.B. The event did not take place in 2020 due to the COVID-19 pandemic
Figure 4 and Table 1 shows the efficiency of the event medical team as only an extremely small percentage of patients that they see get referred to the local ED. Overall, the vast majority of patients are seen and discharged pre-hospitally.
Figure 4. Graph Representing the Number of Patients Seen by the Event Medical Team and the Number of Patients they Refer to Hospital
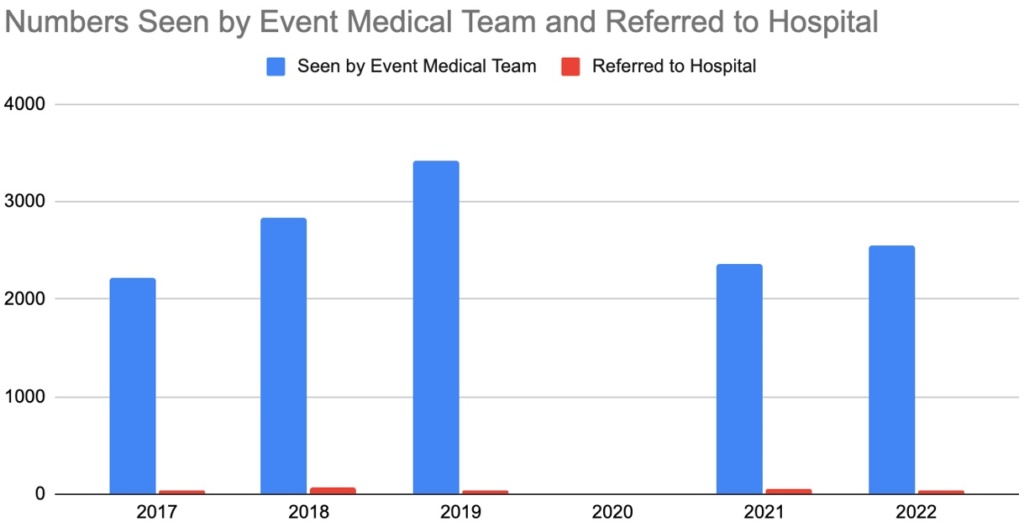
N.B. The event did not take place in 2020 due to the COVID-19 pandemic
| Table 1. Breakdown of the Numbers of Patients Seen by the Event Medical Team, the Number Referred to Hospital and a Percentage of the Numbers |
| Year |
2017 |
2018 |
2019 |
2020 |
2021 |
2022 |
| Seen by the event medical team |
2225 |
2829 |
3424 |
|
2354 |
2554 |
| Referred to hospital |
44 |
63 |
42 |
|
58 |
44 |
| Percentage |
1.98 |
2.23 |
1.23 |
|
2.46 |
1.72 |
| N.B. The event did not take place in 2020 due to the COVID-19 pandemic |
DISCUSSION
Prior to having an established medical service at the event, patients from the event relied solely on the local ED for any medical attention. Therefore, as a direct result of the event, there was a significant increase in the number of patients attending the local ED over the event weekend. This accounted for approximately 10% of ED attendances on the busiest days, placing a strain on the local ED as staffing numbers remained the same and measures had not been put in place to manage the extra patient load. Analysis of the hospital data from 2013 has brought about meaningful changes to help manage patients safely.
With drugs and alcohol being commonly involved, the acuity of patients presenting to ED was variable. Some patients simply required time to sober up, some patients required interventions such as cardioversion for arrhythmias, whereas some required intubation and admission to intensive care. This did increase the pressure on the department as several of the unwell patients required hours of labour intensive care from doctors and nurses in ED to stabilise them. Safeguarding was another aspect to consider with young patients presenting with drugs and alcohol use and concerns were reported to the appropriate safeguarding leads.
All patients seen by the event medical team were pre-alerted to the local ED if they were being sent to hospital, and these patients came with detailed pre-hospital notes. This collaboration between the pre-hospital and multi-disciplinary team in the hospital was crucial to manage the complexity and volume of patients.
To ensure concise communication and continuity of care when these patients returned home from Berkshire, discharge letters from ED were written with clear documentation of their clinical course, advice and follow-up.
LIMITATIONS
Analysis of hospital data commenced in 2013. Unfortunately, it has not been possible to obtain hospital data of the event prior to 2013. The event medical team has been working at the event since 1993. Therefore, a limitation of this research letter is that data prior to 1993 and data between 1993 to 2012 was not analysed. Moreover, the trend and number of patients presenting to ED has changed significantly in the last few years. In 2013, the total ED attendances per day was less than 300. Currently in 2023, we are seeing days where there are in excess of 500 patients presenting to ED. Therefore, the pressures faced by ED over the last few years have grown.
CONCLUSION
To summarise, the measures that were successfully put in place to mitigate the impact on the local ED included:
A medical crew is present at all major events. Teaching nurses and doctors are available to handle minor injuries and toxidromes, for instance and more doctors, nurses, and emergency nurse practitioners are deployed in the emergency department, especially during late nights.6
To provide better service, X-ray and minor injury services have been introduced and the communication between ED and the event medical services have been improved.
Data from 2021 revealed that 2354 patients were seen by the event medical team and only 77 patients were seen in ED from the event (3%). The great majority of attendees seeking medical attention were seen by the on-site medical service and only a small fraction were sent to the local ED. Therefore, this shows that having an established and dynamic medical team at large-scale events and the measures put in place over the years has reduced the impact this event previously had on the local ED.


